Department of Ophthalmology, Interdepartmental Programs, David Geffen Medical School, University of California, Los Angeles, Los Angeles, California, USA.
Department of Ophthalmology, Interdepartmental Programs, David Geffen Medical School, University of California, Los Angeles, Los Angeles, California, USA; Department of Neurology, Interdepartmental Programs, David Geffen Medical School, University of California, Los Angeles, Los Angeles, California, USA; Department of Neuroscience, Interdepartmental Programs, David Geffen Medical School, University of California, Los Angeles, Los Angeles, California, USA; Department of Biomedical Engineering, Interdepartmental Programs, David Geffen Medical School, University of California, Los Angeles, Los Angeles, California, USA.
Am J Ophthalmol. 2020 Aug;216:186-192. doi: 10.1016/j.ajo.2020.03.033. Epub 2020 Apr 2.
Magnetic resonance imaging was used to determine the effect of axial length (AL) on globe rotational axis and horizontal extraocular muscle leverage during horizontal duction.
Prospective observational case series.
At a single academic center, 36 orthophoric adults with a wide range of ALs underwent high-resolution axial orbital magnetic resonance imaging in target-controlled adduction and abduction. ALs were measured in planes containing maximum globe cross-sections. Area centroids were calculated to determine globe centers. Rotational axes in orbital coordinates were calculated from displacements of lens centers and globe-optic nerve attachments. Lever arms were calculated as distances between published extraocular muscle insertions and rotational axes.
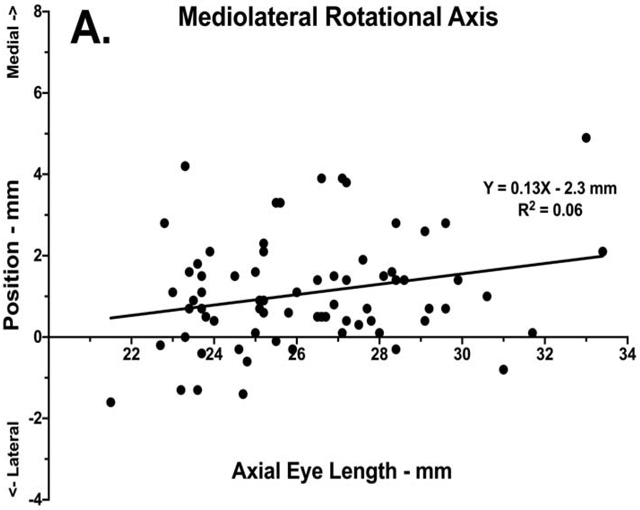
ALs averaged 26.3 ± 0.3 mm (standard error [range 21.5-33.4 mm]). Rotational axes from adduction to abduction averaged 1.1 ± 0.2 mm medial and 1.1 ± 0.2 mm anterior to the globe's geometric center in adduction. Linear regression demonstrated no significant correlation between AL and rotational axis horizontal (R = 0.06) or anteroposterior (R = 0.07) position. Medial rectus (MR) lever arms averaged 12.0 ± 0.2 mm and lateral rectus (LR) lever arms averaged 12.8 ± 0.2 mm. Both MR (R = 0.24, P < .001) and LR (R = 0.32, P < .001) lever arms significantly increased by about 0.3 mm per 1.0-mm of increased AL, with a corresponding reduction in predicted per-millimeter effect of surgical repositioning of their insertions.
Regardless of AL, the globe rotates about a point nasal and anterior to its geometric center, giving the LR more leverage than the MR. This eccentricity may diminish the effect of tendon repositioning in moderate to highly myopic patients, with reductions in per-mill imeter dose/response predicted with longer AL.
磁共振成像(MRI)用于确定眼球旋转轴和水平直肌在水平牵引时的眼外肌杠杆作用与眼轴(AL)的关系。
前瞻性观察性病例系列。
在一个学术中心,36 名具有广泛 AL 的正位成年人在目标控制内收和外展下接受高分辨率眼眶轴向 MRI。在包含眼球最大横截面的平面上测量 AL。通过计算面积质心来确定眼球中心。从晶状体中心和眼球视神经附着点的位移计算轨道坐标中的旋转轴。将肌止点和旋转轴之间的距离计算为肌杠杆臂。
AL 的平均值为 26.3 ± 0.3mm(标准误差[范围 21.5-33.4mm])。从内收到外展的旋转轴平均在内收时向眼球几何中心内侧和前侧 1.1 ± 0.2mm。线性回归显示 AL 与旋转轴水平(R = 0.06)或前后(R = 0.07)位置无显著相关性。内直肌(MR)杠杆臂的平均值为 12.0 ± 0.2mm,外直肌(LR)杠杆臂的平均值为 12.8 ± 0.2mm。MR(R = 0.24,P <.001)和 LR(R = 0.32,P <.001)的杠杆臂都随着 AL 增加约 1.0mm 而增加约 0.3mm,相应地降低了其插入物重新定位的每毫米预测效果。
无论 AL 如何,眼球都绕着其几何中心的鼻侧和前侧旋转,使 LR 的杠杆作用大于 MR。这种偏心度可能会降低在中度至高度近视患者中肌腱重新定位的效果,随着 AL 的延长,预测每毫米剂量/反应的减少。