Furubayashi Nobuki, Negishi Takahito, Takamatsu Dai, Ieiri Kosuke, Inoue Tomohiro, Tsukino Keiji, Nakamura Motonobu
Department of Urology, National Hospital Organization Kyushu Cancer Center, Fukuoka 811-1395, Japan.
Oncol Lett. 2020 Apr;19(4):2943-2949. doi: 10.3892/ol.2020.11368. Epub 2020 Feb 5.
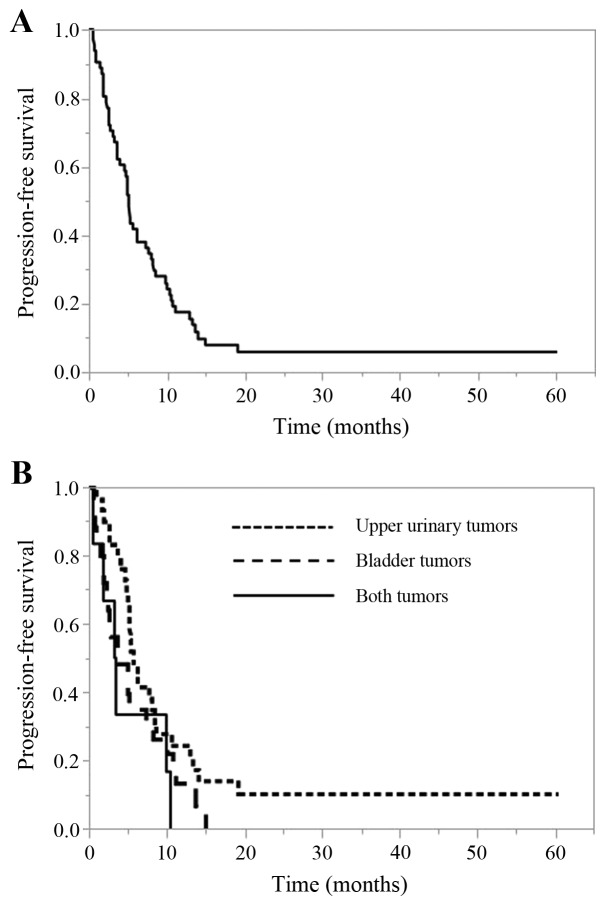
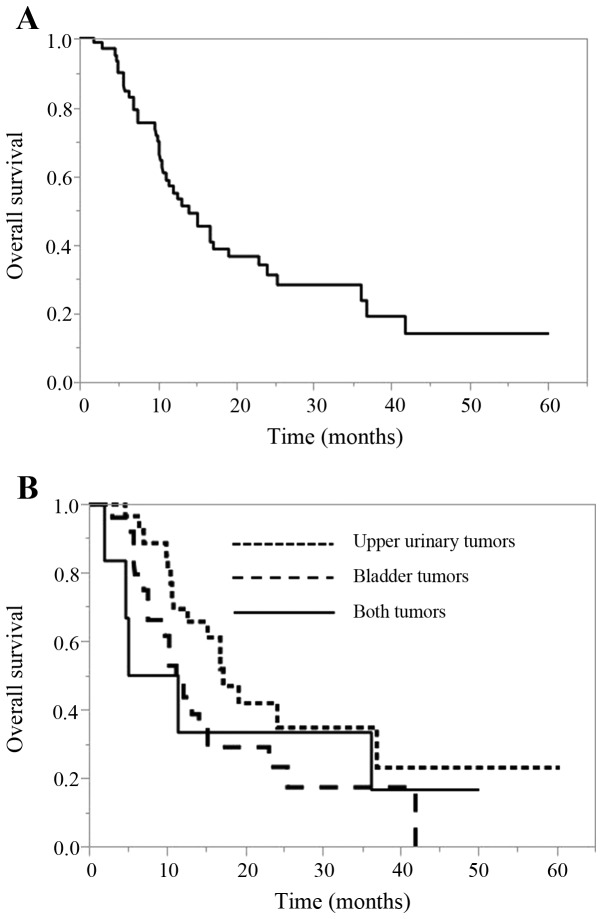
Cisplatin-based systemic chemotherapy is the gold-standard approach for the first-line treatment of patients with advanced or metastatic urothelial carcinoma (UC). However, the optimal number of cycles is still unclear. The current study retrospectively assessed the clinical outcome in patients who received gemcitabine and cisplatin (GC) chemotherapy as first-line treatment for metastatic urothelial cancer to clarify the timing of switching from GC therapy. A total of 61 patients with locally advanced or metastatic UC who received first-line chemotherapy with GC were retrospectively reviewed at National Hospital Organization Kyushu Cancer Center between June 2009 and August 2017. The progression-free survival (PFS) and overall survival (OS) were evaluated using the Kaplan-Meier method. The significance of associations between the clinical parameters and OS was assessed using the Cox proportional hazards regression model. The median cycle number for GC chemotherapy was 4. The median PFS and OS of all cases was 5.2 and 14.1 months, respectively. The multivariate analyses revealed that a neutrophil-to-lymphocyte ratio ≥3.0 (hazard ratio [HR], 2.521, 95% confidence interval [CI]=1.179-5.624; P=0.017) and best response to GC therapy of CR+PR (HR 0.110; 95% CI=0.028-0.411; P<0.001) were independent prognostic factors. However, the number of GC cycles (≤4 vs. >4) was not an independent prognostic factor (P=0.387). The current retrospective study indicated that changes to therapy should be considered at an early stage for cases with a therapeutic effect of SD or less, regardless of the number of GC therapy cycles.
以顺铂为基础的全身化疗是晚期或转移性尿路上皮癌(UC)患者一线治疗的金标准方法。然而,最佳化疗周期数仍不明确。本研究回顾性评估了接受吉西他滨和顺铂(GC)化疗作为转移性尿路上皮癌一线治疗患者的临床结局,以明确从GC治疗转换的时机。2009年6月至2017年8月期间,在九州癌症中心国立医院组织对61例接受GC一线化疗的局部晚期或转移性UC患者进行了回顾性分析。采用Kaplan-Meier法评估无进展生存期(PFS)和总生存期(OS)。使用Cox比例风险回归模型评估临床参数与OS之间关联的显著性。GC化疗的中位周期数为4。所有病例的中位PFS和OS分别为5.2个月和14.1个月。多因素分析显示,中性粒细胞与淋巴细胞比值≥3.0(风险比[HR],2.521,95%置信区间[CI]=1.179-5.624;P=0.017)以及GC治疗的最佳反应为CR+PR(HR 0.110;95%CI=0.028-0.411;P<0.001)是独立的预后因素。然而,GC周期数(≤4 vs.>4)不是独立的预后因素(P=0.387)。当前的回顾性研究表明,对于治疗效果为稳定或更差的病例,无论GC治疗周期数多少,都应尽早考虑改变治疗方案。