Grant Philip, Shumbusho Fabienne, Van Nuil Jennifer Ilo, Kateera Fredrick, Mukherjee Joia, Kabahizi Jules, Ntaganda Fabien, Nsanzimana Sabin, Mbituyumuremyi Aimable, Damascene Makuza Jean, Muvunyi Claude Mambo, Mukabatsinda Constance, Musabeyezu Emmanuel, Ntirenganya Cyprien, Gupta Neil
Division of Infectious Diseases Stanford University Palo Alto CA.
College of Medicine and Health Sciences University of Rwanda Kigali Rwanda.
Hepatol Commun. 2020 Feb 4;4(4):569-576. doi: 10.1002/hep4.1482. eCollection 2020 Apr.
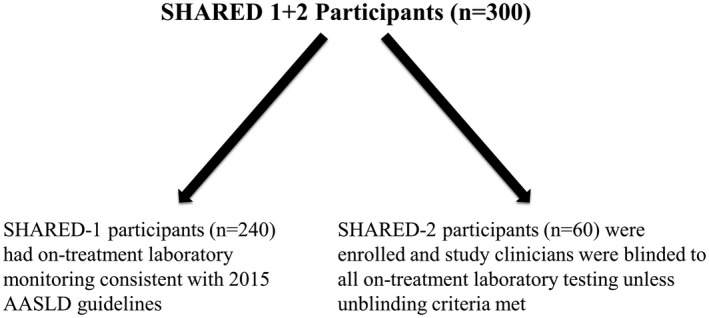
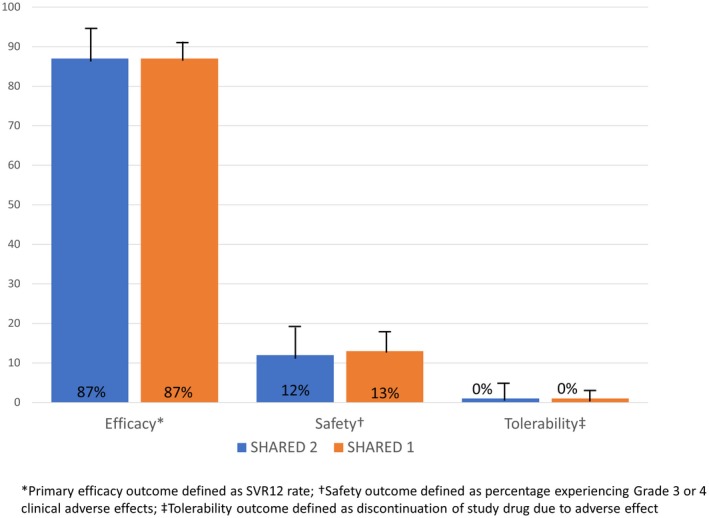
Direct-acting antivirals for hepatitis C virus (HCV) are highly effective and well-tolerated. However, only a small percentage of HCV-infected individuals globally have received therapy. Reducing the complexity of monitoring during HCV therapy, if shown to be safe, could facilitate greater access to HCV services, particularly in resource-limited settings such as sub-Saharan Africa. We enrolled a total of 300 patients who were chronically infected with genotype 4 HCV in Rwanda and treated them with fixed-dose ledispasvir/sofosbuvir for 12 weeks. For 60 consecutive participants enrolled, we blinded the study clinician to on-treatment laboratory results. We compared the efficacy, safety, and tolerability in those with blinded laboratory results to those with standard laboratory monitoring. Baseline characteristics among those with blinded laboratory values were comparable to those with standard monitoring. Among both groups, the median age was 63 years, and the median HCV viral load was 5.9 log (versus 64 years and 6.0 log, respectively). Sustained virologic response rates at 12 weeks after treatment completion were similar in those with blinded laboratories (87%) compared to those with standard laboratory monitoring (87%). There was no increase in adverse events in those with blinded laboratory results, and no participants discontinued the study medication because of an adverse event. On-treatment laboratory monitoring did not improve patient outcomes in those treated with ledispasvir/sofosbuvir. Eliminating this monitoring in treatment programs in resource-limited settings may facilitate and accelerate scale-up of HCV therapy.
丙型肝炎病毒(HCV)直接抗病毒药物疗效显著且耐受性良好。然而,全球范围内仅有一小部分HCV感染者接受了治疗。若能证明减少HCV治疗期间监测的复杂性是安全的,那么将有助于更多人获得HCV治疗服务,尤其是在撒哈拉以南非洲等资源有限的地区。我们在卢旺达共招募了300例慢性感染4型HCV的患者,用固定剂量的来迪派韦/索磷布韦治疗他们12周。对于连续入组的60名参与者,我们对研究临床医生隐瞒治疗期间的实验室检查结果。我们比较了隐瞒实验室检查结果者与接受标准实验室监测者的疗效、安全性和耐受性。隐瞒实验室检查结果者的基线特征与接受标准监测者相当。两组的中位年龄均为63岁,HCV病毒载量中位数分别为5.9 log(标准监测组为64岁和6.0 log)。治疗结束12周时,隐瞒实验室检查结果者的持续病毒学应答率(87%)与接受标准实验室监测者相似(87%)。隐瞒实验室检查结果者的不良事件并未增加,也没有参与者因不良事件而停用研究药物。对于接受来迪派韦/索磷布韦治疗的患者,治疗期间的实验室监测并未改善患者预后。在资源有限地区的治疗项目中取消这种监测可能有助于并加速HCV治疗的推广。