Palsson Ragnar, Short Samuel A P, Kibbelaar Zoe A, Amodu Afolarin, Stillman Isaac E, Rennke Helmut G, McMahon Gearoid M, Waikar Sushrut S
Renal Division, Brigham and Women's Hospital, Boston, Massachusetts, USA.
Division of Nephrology, National University Hospital of Iceland, Reykjavik, Iceland.
Kidney Int Rep. 2020 Mar 4;5(4):511-518. doi: 10.1016/j.ekir.2020.01.012. eCollection 2020 Apr.
The major risk of kidney biopsy is severe bleeding. Numerous risk factors for bleeding after biopsy have been reported, but findings have been inconsistent.
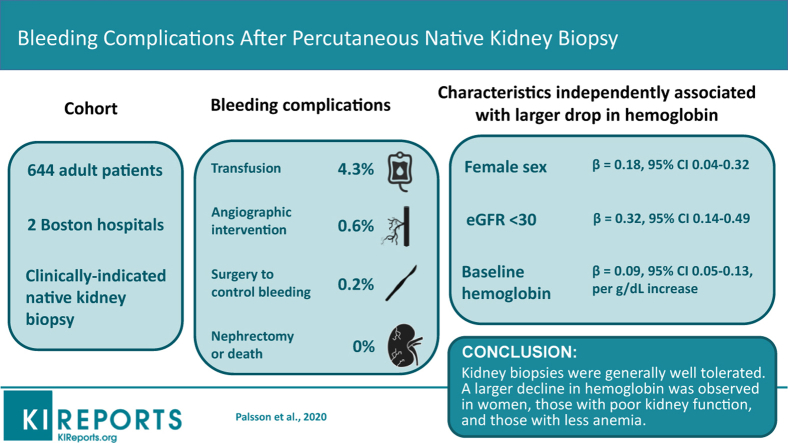
We retrospectively reviewed medical records of adult patients enrolled in a native kidney biopsy cohort study to identify major bleeding events (red blood cell [RBC] transfusions, invasive procedures, kidney loss, or death). We used logistic and linear regression models to identify characteristics associated with postbiopsy RBC transfusions and decline in hemoglobin within a week after the procedure.
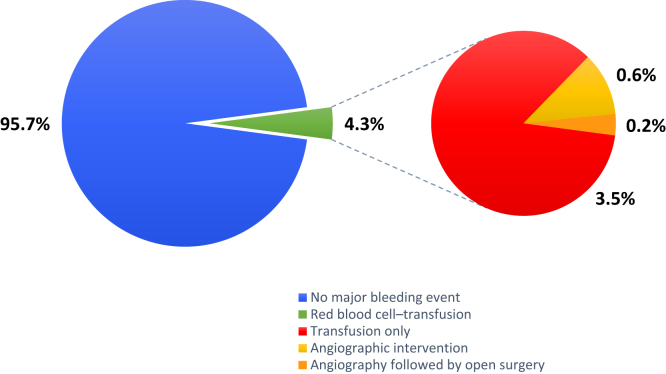
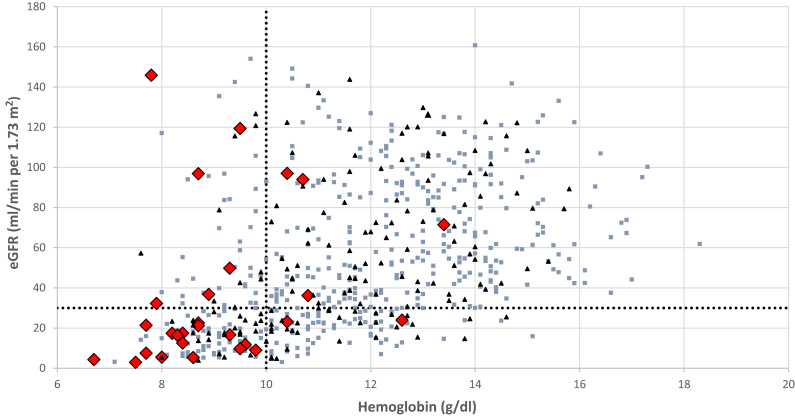
Major bleeding events occurred in 28 of 644 (4.3%) patients (28 required an RBC transfusion, 4 underwent angiographic intervention, and 1 had open surgery to control bleeding). No patient lost a kidney or died because of the biopsy. Postbiopsy RBC transfusion risk was driven by the baseline hemoglobin level (odds ratio [OR] 13.6; 95% confidence interval [CI] 5.4-34.1 for hemoglobin <10 vs. ≥10 g/dl). After adjusting for hemoglobin, no other patient characteristics were independently associated with RBC transfusions. Female sex (β = 0.18; 95% CI: 0.04-0.32), estimated glomerular filtration rate (eGFR) <30 ml/min per 1.73 m (β = 0.32; 95% CI: 0.14-0.49), and baseline hemoglobin (β = 0.09; 95% CI: 0.05-0.13, per g/dl increase) were independently associated with a larger drop in hemoglobin. Histopathologic lesions were not independently associated with major bleeding after biopsy.
Biopsies were generally well tolerated. Baseline hemoglobin was the dominant risk factor for RBC transfusions, but female sex and eGFR <30 ml/min per 1.73 m were also associated with a larger decline in hemoglobin after the procedure.
肾活检的主要风险是严重出血。已有众多关于活检后出血的风险因素报道,但研究结果并不一致。
我们回顾性分析了纳入一项自体肾活检队列研究的成年患者的病历,以确定主要出血事件(红细胞[RBC]输血、侵入性操作、肾丢失或死亡)。我们使用逻辑回归和线性回归模型来确定与活检后RBC输血及术后一周内血红蛋白下降相关的特征。
644例患者中有28例(4.3%)发生主要出血事件(28例需要RBC输血,4例接受血管造影介入治疗,1例接受开放手术控制出血)。没有患者因活检而失去肾脏或死亡。活检后RBC输血风险受基线血红蛋白水平驱动(血红蛋白<10与≥10 g/dl相比,优势比[OR]为13.6;95%置信区间[CI]为5.4 - 34.1)。在对血红蛋白进行校正后,没有其他患者特征与RBC输血独立相关。女性(β = 0.18;95% CI:0.04 - 0.32)、估计肾小球滤过率(eGFR)<30 ml/min/1.73 m²(β = 0.32;95% CI:0.14 - 0.49)和基线血红蛋白(β = 0.09;95% CI:0.05 - 0.13,每增加1 g/dl)与血红蛋白更大幅度下降独立相关。组织病理学病变与活检后主要出血无独立相关性。
活检一般耐受性良好。基线血红蛋白是RBC输血的主要危险因素,但女性和eGFR<30 ml/min/1.73 m²也与术后血红蛋白更大幅度下降相关。