American Board of Internal Medicine, Philadelphia, Pennsylvania.
Department of Economics, Hunter College, New York, New York.
JAMA Netw Open. 2020 Apr 1;3(4):e202494. doi: 10.1001/jamanetworkopen.2020.2494.
Use of health care services and physician practice patterns have been shown to vary widely across the United States. Although practice patterns-in particular, physicians' ability to provide high-quality, high-value care-develop during training, the association of a physician's regional practice environment with that ability is less well understood.
To examine the association between health care intensity in the region where physicians practice and their ability to practice high-value care, specifically for physicians whose practice environment changed due to relocation after residency.
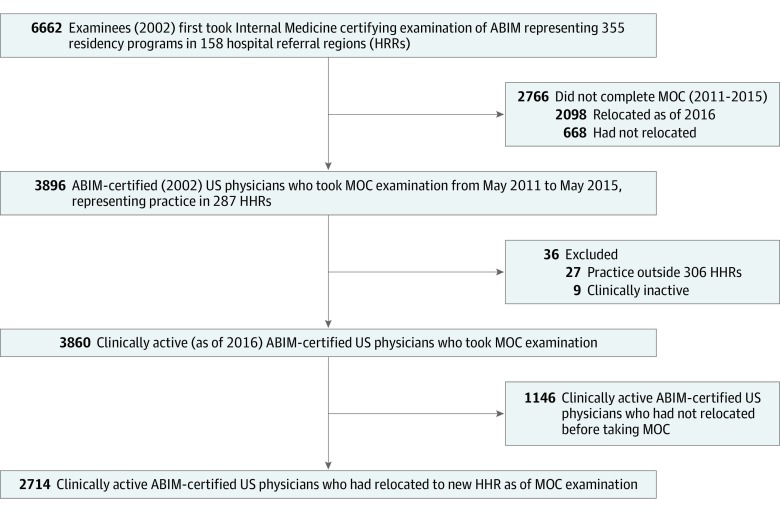
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included a national sample of 3896 internal medicine physicians who took the 2002 American Board of Internal Medicine initial certification examination followed approximately 1 decade (April 21, 2011, to May 7, 2015) later by the Maintenance of Certification (MOC) examination. At the time of the MOC examination, 2714 of these internists were practicing in a new region. Data were analyzed from March 6, 2016, to May 21, 2018.
Intensity of care in the Dartmouth Atlas hospital referral region (HRR), measured by per-enrollee end-of-life physician visits (primary) and current practice type (secondary).
The outcome, a physician's ability to practice high-value care, was assessed using the Appropriately Conservative Management (ACM) score on the MOC examination, measuring performance across all questions for which the correct answer was the most conservative option. The exposure, regional health care intensity, was measured as per-enrollee end-of-life physician visits in the Dartmouth Atlas HRR of the physician's practice.
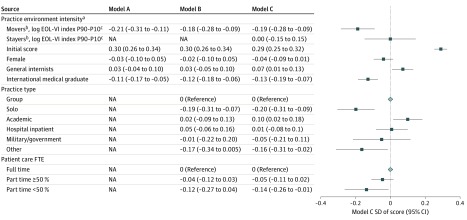
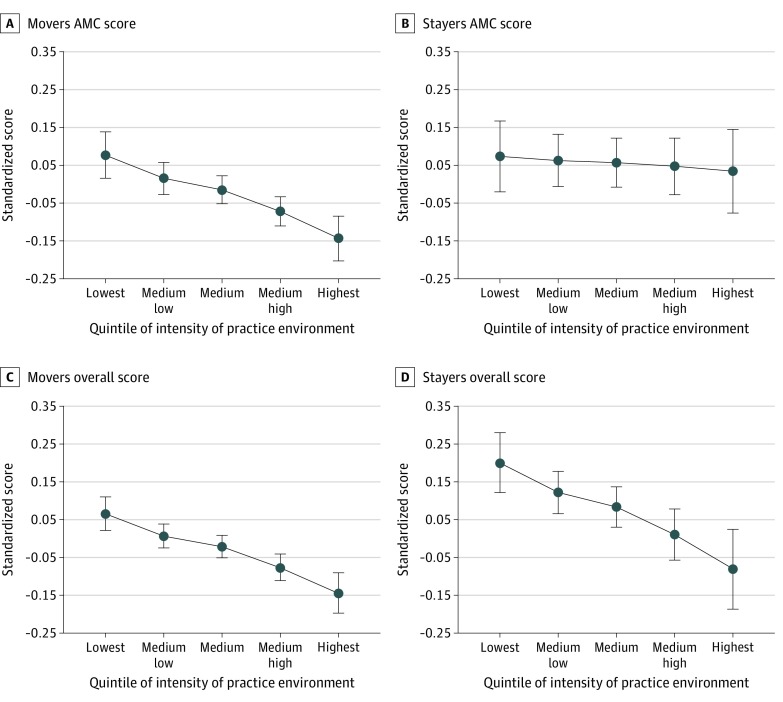
Among the 3860 participating internists included in the analysis (2030 men [52.6%]; mean [SD] age, 45.6 [4.5] years), those who moved to regions in the quintile of highest health care intensity had an ACM score 0.22 SD lower (95% CI, -0.32 to -0.12) than internists who moved to regions in the quintile of lowest intensity, controlling for postresidency ACM scores. This difference reflected scoring in the 44th compared with the 53rd percentile of all examinees. This association was mildly attenuated (0.18 SD less; 95% CI, -0.28 to -0.09) after adjustment for physician and practice characteristics.
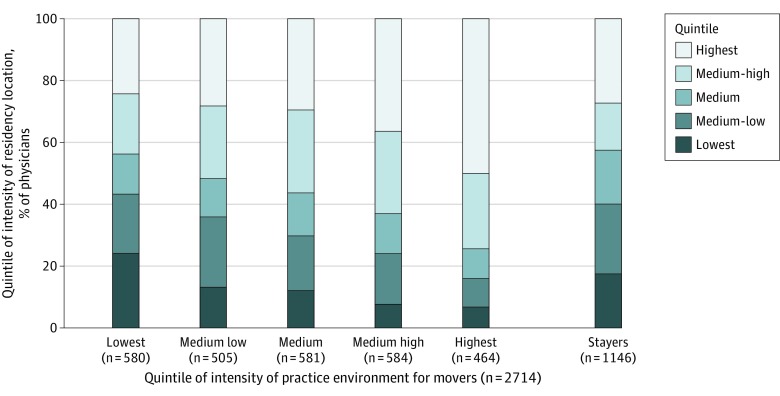
This study found that practice patterns of internists who relocate after residency training appear to migrate toward norms of the new region. The demands of practicing in high-intensity regions may erode the ability to practice high-value conservative care.
在美国,医疗服务的使用和医生的实践模式差异很大。尽管实践模式——特别是医生提供高质量、高价值医疗服务的能力——是在培训过程中发展起来的,但医生所在地区的实践环境与这种能力的关联却不太为人所知。
研究医生所在地区的医疗保健强度与他们提供高价值医疗服务的能力之间的关系,特别是对于那些因住院医师培训后搬迁而改变实践环境的医生。
设计、地点和参与者:这项队列研究包括了全国范围内 3896 名内科医生的样本,他们参加了 2002 年美国内科委员会的初始认证考试,大约 10 年后(2011 年 4 月 21 日至 2015 年 5 月 7 日),他们参加了维持认证(MOC)考试。在 MOC 考试时,这些内科医生中有 2714 人在新的地区行医。数据来自 2016 年 3 月 6 日至 2018 年 5 月 21 日。
达特茅斯地图集医院转诊区(HRR)的护理强度,通过每位患者临终前的医生就诊次数(主要)和当前的实践类型(次要)来衡量。
作为医生提供高价值医疗服务能力的指标,使用 MOC 考试中的适当保守管理(ACM)评分来评估,该评分衡量了所有正确答案为最保守选项的问题的表现。暴露,即医生所在地区的区域医疗保健强度,通过医生所在地区的达特茅斯地图集 HRR 中每位患者临终前的医生就诊次数来衡量。
在参与分析的 3860 名内科医生中(2030 名男性[52.6%];平均[标准差]年龄为 45.6[4.5]岁),与搬到医疗保健强度最低的五分位区的内科医生相比,搬到医疗保健强度最高的五分位区的内科医生的 ACM 评分低 0.22 个标准差(95%置信区间,-0.32 至-0.12),这一差异反映了在所有考生中排在第 44 位与第 53 位之间的差距。这种关联在调整住院医师培训后的 ACM 评分后有所减弱(低 0.18 个标准差;95%置信区间,-0.28 至-0.09)。
这项研究发现,住院医师培训后搬迁的内科医生的实践模式似乎向新地区的规范靠拢。在高强度地区行医的需求可能会削弱提供高价值保守治疗的能力。