Serra Joao Tiago, Mueller Johannes, Teng Haidong, Elshaarawy Omar, Mueller Sebastian
Center for Alcohol Research, University of Heidelberg and Salem Medical Center, Heidelberg, Baden-Württemberg, Germany.
Hepat Med. 2020 Mar 27;12:41-48. doi: 10.2147/HMER.S245455. eCollection 2020.
Transient elastography (TE) using FibroScan (FS) has been established to non-invasively assess liver fibrosis and steatosis. The aim of this study was to compare the recently introduced FibroTouch (FT) device with the established FS with respect to liver stiffness and CAP.
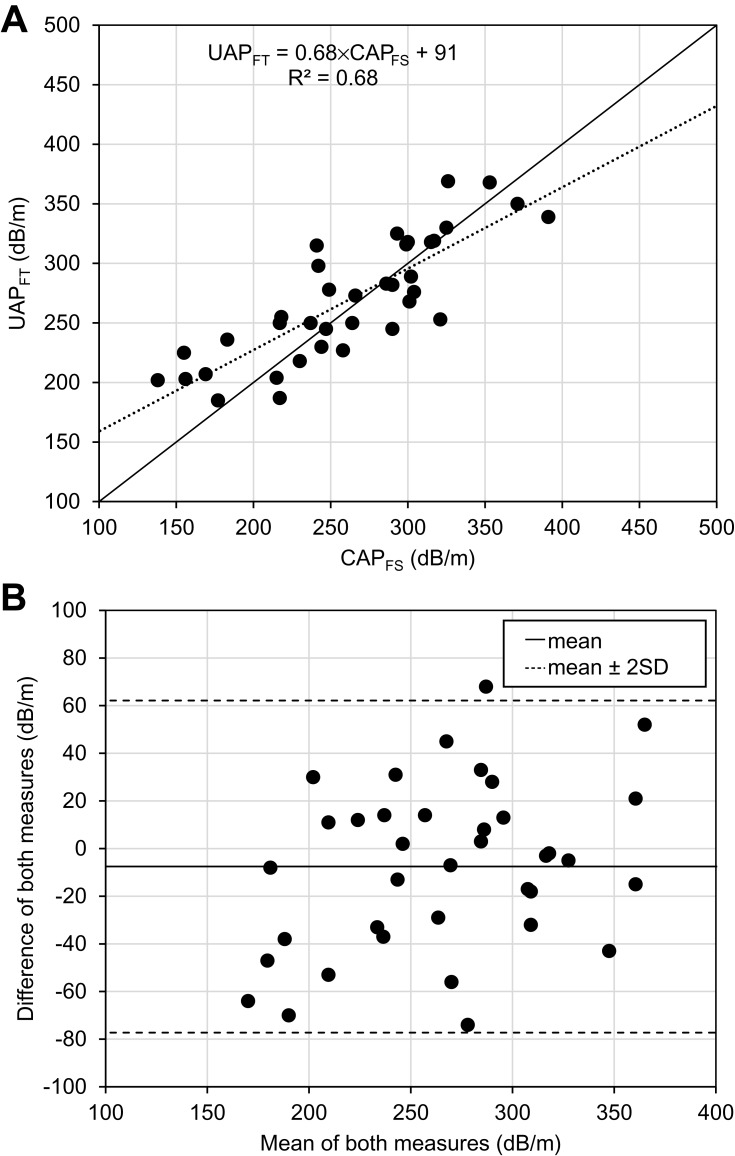
Thirty-nine patients with and without liver disease were included. All patients were measured three times with FS (FibroScan 530 compact, Echosens, France) and FT (FibroTouch-FT100, Wuxi Hisky Med, China). For FS, M and XL probe were used according to the manufacturer's specifications. For steatosis, CAP and the comparable FT equivalent UAP (ultrasound attenuation parameter) was determined. Finally, FT and FS were explored in liver tissue-mimicking phantoms.
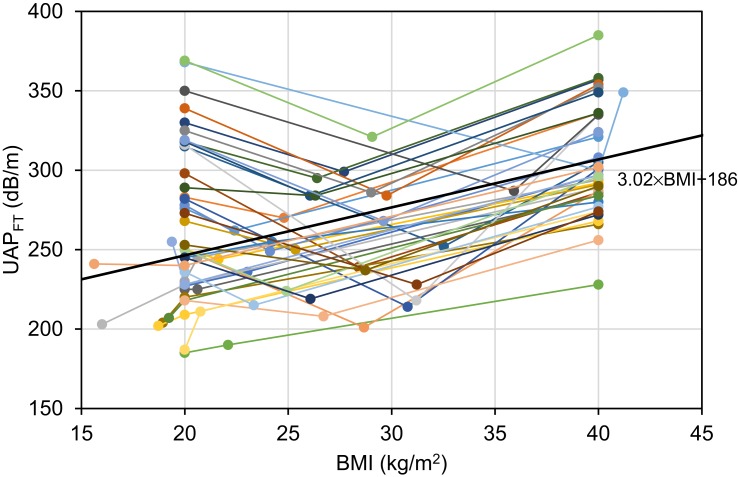
LS between FS and FT correlated well with r=0.91. Root-mean-square (RMS) of the coefficient of variation for LS was better in FS (11.1% vs 27.4%). Bland-Altman analysis showed a 3.1 kPa mean overestimation of LS by FT. In addition, UAP strongly and linearly depended on the BMI following UAP=3.02 × BMI+186. In phantoms, a similar relation was found with UAP (phantom)= 3.78 × BMI + 146 suggesting that UAP is directly calculated from entered BMI instead of assessing shear-wave attenuation. Consequently, RMS-CV was lower for FT (6.0% vs 9.7%). However, if using different BMI, CV-RMS for FT increased to 12.7%. LS of a patient with manifest liver cirrhosis and ascites was 38.8 kPa using the FS-XL probe but almost normal with FT (7.2 kPa).
Although LS by FT shows good correlation with LS-FS, it has larger variation, continuously overestimates LS and completely fails in ascites. Moreover, FT-UAP seems to be a misleading parameter for steatosis assessment because it is at least in part calculated from mandatory entered patient data. In conclusion, novel LS cut-off values need to be defined for LS-FT and usage of UAP is not recommended.
已采用FibroScan(FS)的瞬时弹性成像(TE)技术来无创评估肝纤维化和脂肪变性。本研究的目的是比较最近推出的FibroTouch(FT)设备与已有的FS设备在肝脏硬度和受控衰减参数(CAP)方面的差异。
纳入39例有或无肝脏疾病的患者。所有患者均使用FS(FibroScan 530 compact,法国Echosens公司)和FT(FibroTouch - FT100,中国无锡海斯凯尔医学技术有限公司)各测量3次。对于FS,根据制造商的规格使用M型和XL型探头。对于脂肪变性,测定CAP以及与之可比的FT等效超声衰减参数(UAP)。最后,在肝脏组织模拟体模中对FT和FS进行了研究。
FS和FT测得的肝脏硬度(LS)相关性良好,r = 0.91。FS测得的LS变异系数的均方根(RMS)更好(11.1%对27.4%)。Bland - Altman分析显示FT测得的LS平均高估3.1 kPa。此外,UAP强烈且线性地依赖于体重指数(BMI),关系式为UAP = 3.02×BMI + 186。在体模中,发现UAP(体模)= 3.78×BMI + 146的类似关系,这表明UAP是根据输入的BMI直接计算得出,而非评估剪切波衰减。因此,FT的RMS - CV较低(6.0%对9.7%)。然而,如果使用不同的BMI,FT的CV - RMS会增至12.7%。一名有明显肝硬化和腹水的患者使用FS - XL探头测得的LS为38.8 kPa,但使用FT测得的结果几乎正常(7.2 kPa)。
尽管FT测得的LS与FS测得的LS显示出良好的相关性,但它的变异较大,持续高估LS,且在腹水情况下完全失效。此外,FT - UAP似乎是脂肪变性评估中的一个误导性参数,因为它至少部分是根据强制输入的患者数据计算得出。总之,需要为FT - LS定义新的截断值,不建议使用UAP。