Natera, Inc., San Carlos, California; and the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, Maryland.
Obstet Gynecol. 2020 May;135(5):1198-1206. doi: 10.1097/AOG.0000000000003791.
To assess the causes of reported discordance between noninvasive prenatal testing (NIPT) and ultrasound or other clinical information.
In this retrospective, observational study, all cases in which single-nucleotide polymorphism (SNP)-based NIPT reported normal sex chromosomes and the laboratory was notified by the patient or health care provider of discordance between NIPT and observed or expected fetal sex from clinical information were reviewed. When discordances were unresolved after internal and external laboratory clerical data review or repeat ultrasound imaging, additional clinical records, genetic testing results and pregnancy outcomes were reviewed.
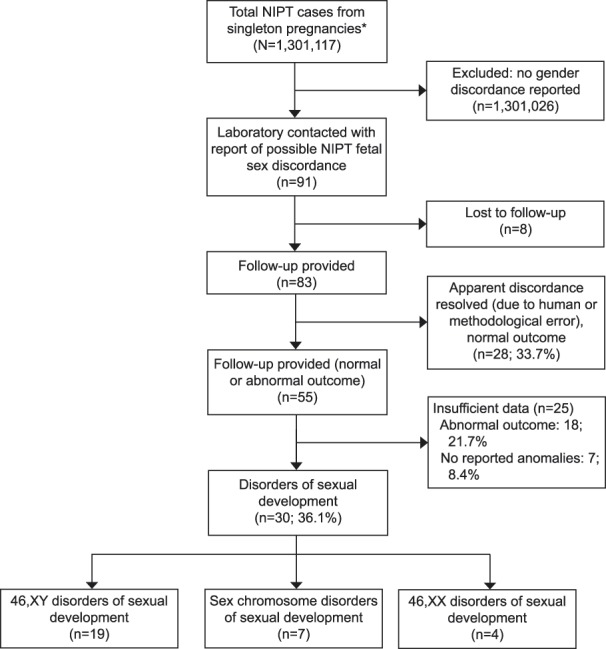
Of the 1,301,117 eligible NIPT cases, fetal sex discordances were reported in 91 (0.007%; 1:14,300; 95% CI 1:11,600-1:17,800); partial or complete outcome information was available for 83 of 91 cases. In 30 of 83 (36%) cases, karyotyping was performed, and sufficient clinical information was provided to establish the diagnosis of disorders of sexual development. The disorders of sexual development were classified into three categories: 46,XY disorders of sexual development (n=19), 46,XX disorders of sexual development (n=4), and sex chromosome disorders of sexual development (n=7). In 28 of 83 (34%) cases, the cause of the apparent discrepancy was attributable to human error, predominantly phlebotomy labeling or ultrasound misassignment. In 25 of 83 cases, a diagnosis was not possible; the outcome reported was either abnormal (18/83, 22%) or no abnormalities were reported (7/83, 8%). When normal sex chromosomes were predicted by SNP-based NIPT and clinical information was discordant, disorders of sexual development were common. Internal laboratory clerical data review and re-imaging confirmed the NIPT fetal sex reports in 34% cases, providing reassurance that no further evaluation was necessary.
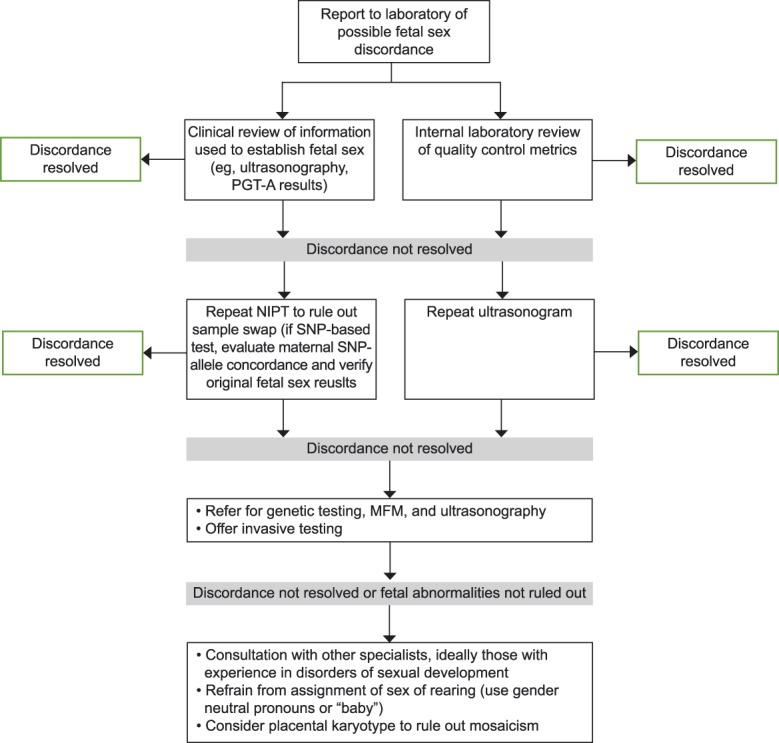
Identification of apparent fetal sex discordances with NIPT results, and reporting this suspicion to the laboratory, provides an opportunity for further evaluation to identify the cause of apparent discordances and the involvement of a multi-disciplinary team, as necessary to prepare for postnatal care. We propose a protocol for evaluation of these cases.
This study was funded by Natera, Inc.
评估无创产前检测(NIPT)与超声或其他临床信息之间报告不一致的原因。
在这项回顾性观察性研究中,对所有报告 SNP 基 NIPT 正常性染色体但患者或医疗保健提供者通知实验室 NIPT 与临床信息观察到或预期的胎儿性别之间存在不一致的病例进行了回顾。当内部和外部实验室文书数据审查或重复超声成像后仍无法解决不一致时,审查了其他临床记录、遗传检测结果和妊娠结局。
在 1301117 例合格的 NIPT 病例中,报告了 91 例(0.007%;1:14300;95%CI 1:11000-1:17800)胎儿性别不一致;91 例中有 83 例提供了部分或完整的结局信息。在 83 例中的 30 例(36%)中进行了核型分析,并提供了足够的临床信息以确立性发育障碍的诊断。性发育障碍分为三类:46,XY 性发育障碍(19 例)、46,XX 性发育障碍(4 例)和性染色体性发育障碍(7 例)。在 83 例中的 28 例(34%)中,明显差异的原因归因于人为错误,主要是采血标签或超声分配错误。在 83 例中的 25 例中,无法做出诊断;报告的结果要么是异常(83 例中的 18 例,22%),要么是无异常(83 例中的 7 例)。当 SNP 基 NIPT 预测正常性染色体且临床信息不一致时,性发育障碍较为常见。内部实验室文书数据审查和重新成像确认了 34%病例中的 NIPT 胎儿性别报告,这提供了保证,表明无需进一步评估。
识别 NIPT 结果中明显的胎儿性别不一致,并将这种怀疑报告给实验室,为进一步评估提供了机会,以确定明显不一致的原因,并在必要时涉及多学科团队,为产后护理做准备。我们提出了一种评估这些病例的方案。
本研究由 Natera,Inc. 资助。