Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, TX.
Roswell Park Comprehensive Cancer Center, Buffalo, NY.
Blood. 2020 Aug 6;136(6):674-683. doi: 10.1182/blood.2019004143.
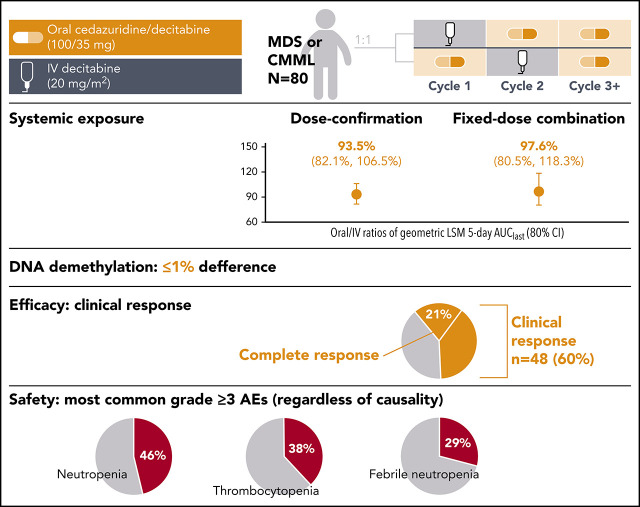
This phase 2 study was designed to compare systemic decitabine exposure, demethylation activity, and safety in the first 2 cycles with cedazuridine 100 mg/decitabine 35 mg vs standard decitabine 20 mg/m2 IV. Adults with International Prognostic Scoring System intermediate-1/2- or high-risk myelodysplastic syndromes (MDS) or chronic myelomonocytic leukemia (CMML) were randomized 1:1 to receive oral cedazuridine/decitabine or IV decitabine in cycle 1, followed by crossover to the other treatment in cycle 2. All patients received oral cedazuridine/decitabine in subsequent cycles. Cedazuridine and decitabine were given initially as separate capsules in a dose-confirmation stage and then as a single fixed-dose combination (FDC) tablet. Primary end points: mean decitabine systemic exposure (geometric least-squares mean [LSM]) of oral/IV 5-day area under curve from time 0 to last measurable concentration (AUClast), percentage long interspersed nuclear element 1 (LINE-1) DNA demethylation for oral cedazuridine/decitabine vs IV decitabine, and clinical response. Eighty patients were randomized and treated. Oral/IV ratios of geometric LSM 5-day AUClast (80% confidence interval) were 93.5% (82.1-106.5) and 97.6% (80.5-118.3) for the dose-confirmation and FDC stages, respectively. Differences in mean %LINE-1 demethylation between oral and IV were ≤1%. Clinical responses were observed in 48 patients (60%), including 17 (21%) with complete response. The most common grade ≥3 adverse events regardless of causality were neutropenia (46%), thrombocytopenia (38%), and febrile neutropenia (29%). Oral cedazuridine/decitabine (100/35 mg) produced similar systemic decitabine exposure, DNA demethylation, and safety vs decitabine 20 mg/m2 IV in the first 2 cycles, with similar efficacy. This study is registered at www.clinicaltrials.gov as #NCT02103478.
这项 2 期研究旨在比较第 1 至 2 周期中系统地西他滨暴露、去甲基化活性和安全性,与 Cedazuridine 100mg/Decitabine 35mg 与标准剂量的 Decitabine 20mg/m2 IV 相比。患有国际预后评分系统中危-1/2 或高危骨髓增生异常综合征(MDS)或慢性粒单核细胞白血病(CMML)的成年人按 1:1 随机分配接受口服 Cedazuridine/Decitabine 或 IV 地西他滨治疗,在第 1 周期中,随后在第 2 周期中交叉至另一种治疗。所有患者在随后的周期中均接受口服 Cedazuridine/Decitabine 治疗。Cedazuridine 和地西他滨最初以单独胶囊的形式在剂量确认阶段给药,然后以单一固定剂量组合(FDC)片剂的形式给药。主要终点:口服/IV 5 天时间曲线下面积的平均地西他滨系统暴露(几何最小二乘均数[LSM])从 0 到最后可测量浓度(AUClast),口服 Cedazuridine/Decitabine 与 IV 地西他滨相比的长散布核元件 1(LINE-1)DNA 去甲基化的百分比,以及临床反应。80 例患者被随机分配并接受治疗。口服/IV 几何 LSM 5 天 AUC(80%置信区间)分别为剂量确认阶段 93.5%(82.1-106.5)和 FDC 阶段 97.6%(80.5-118.3)。口服和 IV 之间平均%LINE-1 去甲基化的差异均≤1%。48 例患者(60%)观察到临床反应,包括 17 例(21%)完全缓解。无论因果关系如何,最常见的≥3 级不良事件是中性粒细胞减少(46%)、血小板减少(38%)和发热性中性粒细胞减少(29%)。口服 Cedazuridine/Decitabine(100/35mg)在第 1 至 2 周期中产生与 IV 地西他滨 20mg/m2 相似的系统地西他滨暴露、DNA 去甲基化和安全性,且疗效相似。这项研究在 www.clinicaltrials.gov 上注册为#NCT02103478。