Department of Respiratory and Critical Care Medicine, Tianjin Chest Hospital, 261, Taierzhuang South Road, Jinnan District, Tianjin, 300222, China.
The clinical laboratory, Tianjin Chest Hospital, Tianjin, 300222, China.
BMC Pulm Med. 2020 Apr 15;20(1):89. doi: 10.1186/s12890-020-1125-y.
At present, serum Aspergillus IgG and IgM antibody detection is mainly used in the diagnosis of chronic pulmonary aspergillosis (CPA), but its value in the diagnosis of invasive pulmonary aspergillosis (IPA) in non-agranulocytic patients is still unclear. IgM can be used as a marker of acute infection to help diagnose acute infection-related diseases. IgG is a marker of long-term infection and is used to assist in the diagnosis of pre-existing or chronic infection-related diseases. The aim of this study was to investigate and compare the value of serum Aspergillus IgG and IgM antibody detection in the diagnosis of IPA and CPA in non-agranulocytic patients.
Fifty-eight cases of pulmonary aspergillosis (37 IPA and 21 CPA cases), 15 cases of community-acquired bacterial pneumonia and 50 cases in the healthy control group were collected. The serum (1,3)-β-D-glucan test (G test) was performed with a chromogenic method, and the galactomannan test (GM test) and Aspergillus IgG and IgM antibody detection were performed by commercial enzyme-linked immunosorbent assay (ELISA) in all patients. The sensitivity and specificity, cut-off value and area under the curve (AUC) of Aspergillus IgG and IgM antibodies were further obtained by receiver operating characteristic (ROC) curves.
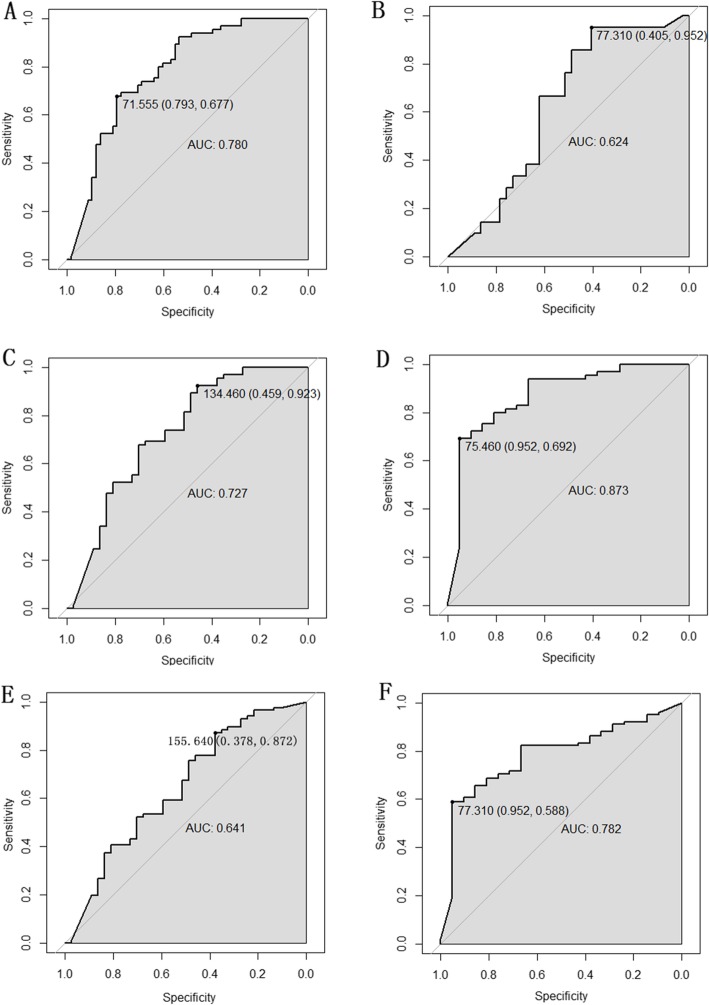
The positive rate of the G test, Aspergillus IgG antibody detection and the GM test also showed notable differences among the IPA, CPA, community-acquired bacterial pneumonia and healthy groups (P = 0.006, P < 0.001 and P = 0.217, respectively). Only the positive rate of the GM test showed a significant difference between the IPA and CPA groups (P = 0.04). ROC curves indicated that Aspergillus IgG antibody detection had a higher specificity in the IPA group than in the CPA group (0.952). The detection of Aspergillus IgG antibody can preferably distinguish IPA from community-acquired bacterial pneumonia and healthy controls (sensitivity = 0.923, specificity = 0.459, cut-off value = 134.46, AUC = 0.727). It can also distinguish CPA from community-acquired bacterial pneumonia and healthy controls (sensitivity = 0.952, specificity = 0.692, cut-off value = 75.46, AUC = 0.873).
Serum Aspergillus IgG antibody detection may have certain clinical value in the diagnosis of IPA and CPA in non-agranulocytic patients.
目前,血清曲霉 IgG 和 IgM 抗体检测主要用于慢性肺曲霉病(CPA)的诊断,但在非粒细胞患者侵袭性肺曲霉病(IPA)的诊断中的价值仍不清楚。IgM 可作为急性感染的标志物,有助于诊断急性感染相关疾病。IgG 是长期感染的标志物,用于辅助诊断既往或慢性感染相关疾病。本研究旨在探讨和比较血清曲霉 IgG 和 IgM 抗体检测在非粒细胞患者 IPA 和 CPA 诊断中的价值。
收集了 58 例肺曲霉病(37 例 IPA 和 21 例 CPA 病例)、15 例社区获得性细菌性肺炎和 50 例健康对照组患者。所有患者均采用显色法进行(1,3)-β-D-葡聚糖试验(G 试验),采用商业酶联免疫吸附试验(ELISA)进行半乳甘露聚糖试验(GM 试验)和曲霉 IgG 和 IgM 抗体检测。通过受试者工作特征(ROC)曲线进一步获得曲霉 IgG 和 IgM 抗体的灵敏度和特异性、临界值和曲线下面积(AUC)。
G 试验、曲霉 IgG 抗体检测和 GM 试验的阳性率在 IPA、CPA、社区获得性细菌性肺炎和健康组之间也存在显著差异(P = 0.006,P < 0.001 和 P = 0.217)。仅 GM 试验的阳性率在 IPA 和 CPA 组之间存在显著差异(P = 0.04)。ROC 曲线表明,曲霉 IgG 抗体检测在 IPA 组中的特异性高于 CPA 组(0.952)。检测曲霉 IgG 抗体可以更好地区分 IPA 与社区获得性细菌性肺炎和健康对照组(灵敏度=0.923,特异性=0.459,临界值=134.46,AUC=0.727)。它还可以区分 CPA 与社区获得性细菌性肺炎和健康对照组(灵敏度=0.952,特异性=0.692,临界值=75.46,AUC=0.873)。
血清曲霉 IgG 抗体检测在非粒细胞患者 IPA 和 CPA 的诊断中可能具有一定的临床价值。