J Int AIDS Soc. 2020 Apr;23(4):e25477. doi: 10.1002/jia2.25477.
Limited data describe outcomes on second-line antiretroviral therapy (ART) among children globally. Our objective was to contribute data on outcomes among children living with HIV after initiation of second-line ART in the context of routine care within a large global cohort collaboration.
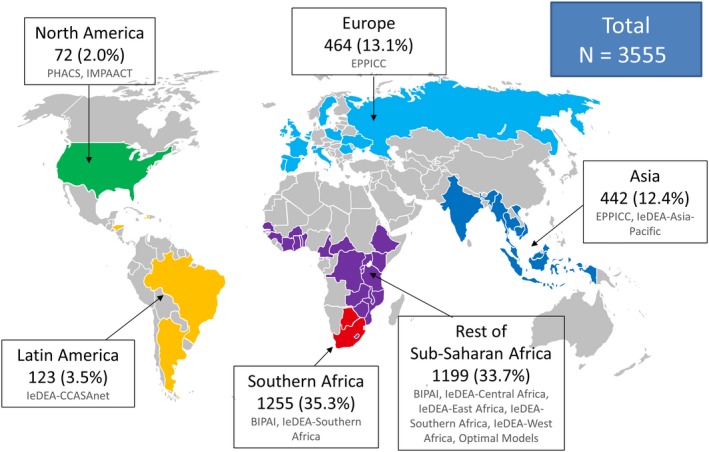
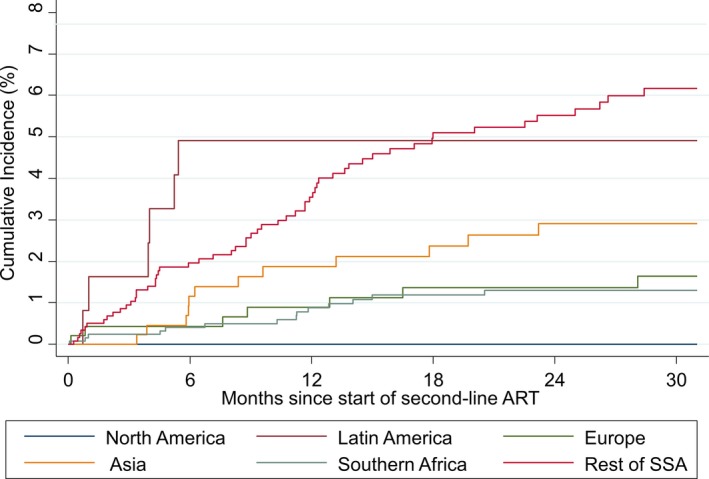
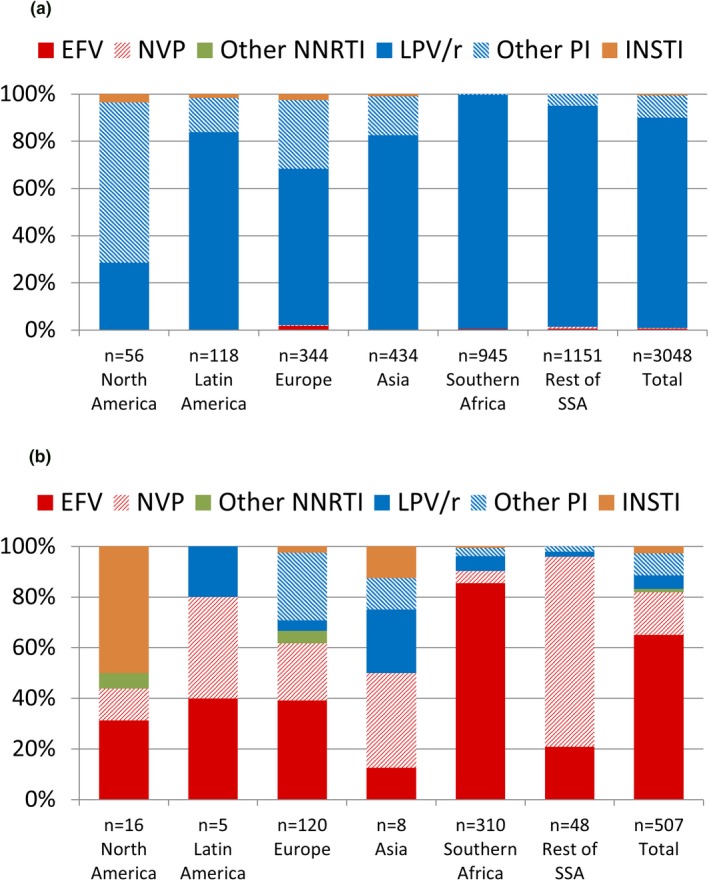
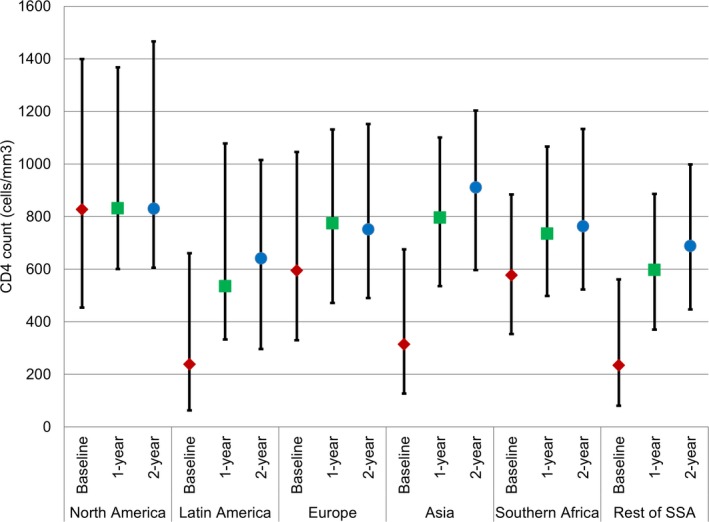
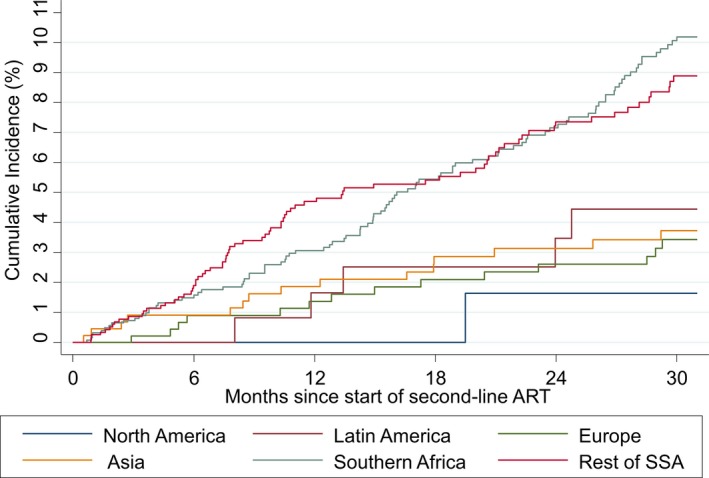
Patient-level data from 1993 through 2015 from 11 paediatric HIV cohorts were pooled. Characteristics at switch and through two years of follow-up were summarized for children who switched to second-line ART after starting a standard first-line regimen in North America, Latin America, Europe, Asia, Southern Africa (South Africa & Botswana) and the rest of sub-Saharan Africa (SSA). Cumulative incidences of mortality and loss to follow-up (LTFU) were estimated using a competing risks framework.
Of the 85,389 children on first-line ART, 3,555 (4%) switched to second-line after a median of 2.8 years on ART (IQR: 1.6, 4.7); 69% were from Southern Africa or SSA and 86% of second-line regimens were protease inhibitor-based. At switch, median age was 8.4 years and 50% had a prior AIDS diagnosis. Median follow-up after switch to second-line ranged from 1.8 years in SSA to 5.3 years in North America. Median CD4 counts at switch to second-line ranged from 235 cells/mm in SSA to 828 cells/mm in North America. Improvements in CD4 counts were observed over two years of follow-up, particularly in regions with lower CD4 counts at second-line switch. Improvements in weight-for-age z-scores were not observed during follow-up. Cumulative incidence of LTFU at two years was <5% in all regions except SSA (7.1%) and Southern Africa (7.4%). Risk of mortality was <3% at two years of follow-up in all regions, except Latin America (4.9%) and SSA (5.5%).
Children switched to second-line ART experience CD4 count increases as well as low to moderate rates of LTFU and mortality within two years after switch. Severe immune deficiency at time of switch in some settings suggests need for improved recognition and management of treatment failure in children.
全球范围内,仅有有限的数据描述了儿童二线抗逆转录病毒治疗(ART)的结果。我们的目的是在大型全球队列合作中,为常规护理背景下开始二线 ART 的儿童提供结果数据。
从 1993 年至 2015 年,来自 11 个儿科 HIV 队列的患者水平数据被汇总。总结了在北美、拉丁美洲、欧洲、亚洲、南部非洲(南非和博茨瓦纳)和撒哈拉以南非洲(SSA)的其余地区,开始标准一线方案后转为二线 ART 的儿童在切换时和两年随访期间的特征。使用竞争风险框架估计死亡率和失访(LTFU)的累积发生率。
在接受一线 ART 的 85389 名儿童中,3555 名(4%)在接受 ART 中位数为 2.8 年(IQR:1.6,4.7)后转为二线;69%来自南部非洲或 SSA,86%的二线方案为蛋白酶抑制剂为基础。切换时,中位年龄为 8.4 岁,50%有先前的艾滋病诊断。从 SSA 的二线切换后中位随访时间为 1.8 年,到北美为 5.3 年。二线切换时的中位 CD4 计数从 SSA 的 235 个细胞/mm 到北美的 828 个细胞/mm。在两年的随访期间,观察到 CD4 计数的改善,特别是在二线切换时 CD4 计数较低的地区。在随访期间,体重与年龄的 Z 评分没有改善。除 SSA(7.1%)和南部非洲(7.4%)外,所有地区两年的 LTFU 累积发生率均<5%。在所有地区,两年的随访期间死亡率风险均<3%,除拉丁美洲(4.9%)和 SSA(5.5%)外。
在二线 ART 中切换的儿童在切换后两年内经历了 CD4 计数的增加,以及较低至中度的 LTFU 和死亡率。在某些情况下,切换时的严重免疫缺陷表明需要改进对儿童治疗失败的识别和管理。