Center for Infectious Diseases Epidemiology and Research, University of Cape Town, Cape Town, South Africa.
Harvard T. H. Chan School of Public Health, Boston, Massachusetts, United States of America.
PLoS Med. 2018 Mar 1;15(3):e1002514. doi: 10.1371/journal.pmed.1002514. eCollection 2018 Mar.
Globally, the population of adolescents living with perinatally acquired HIV (APHs) continues to expand. In this study, we pooled data from observational pediatric HIV cohorts and cohort networks, allowing comparisons of adolescents with perinatally acquired HIV in "real-life" settings across multiple regions. We describe the geographic and temporal characteristics and mortality outcomes of APHs across multiple regions, including South America and the Caribbean, North America, Europe, sub-Saharan Africa, and South and Southeast Asia.
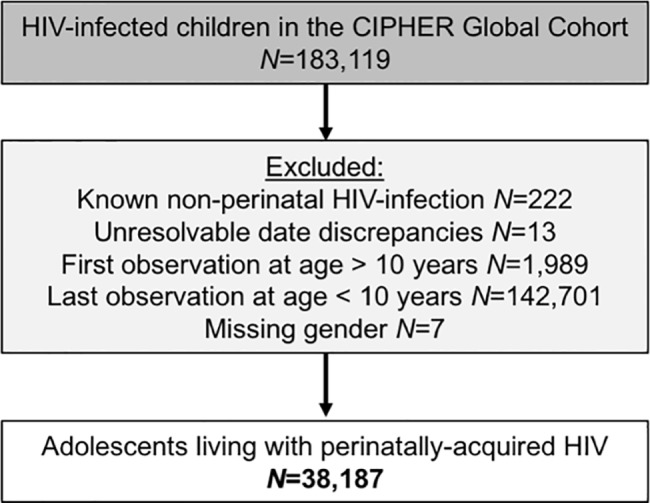
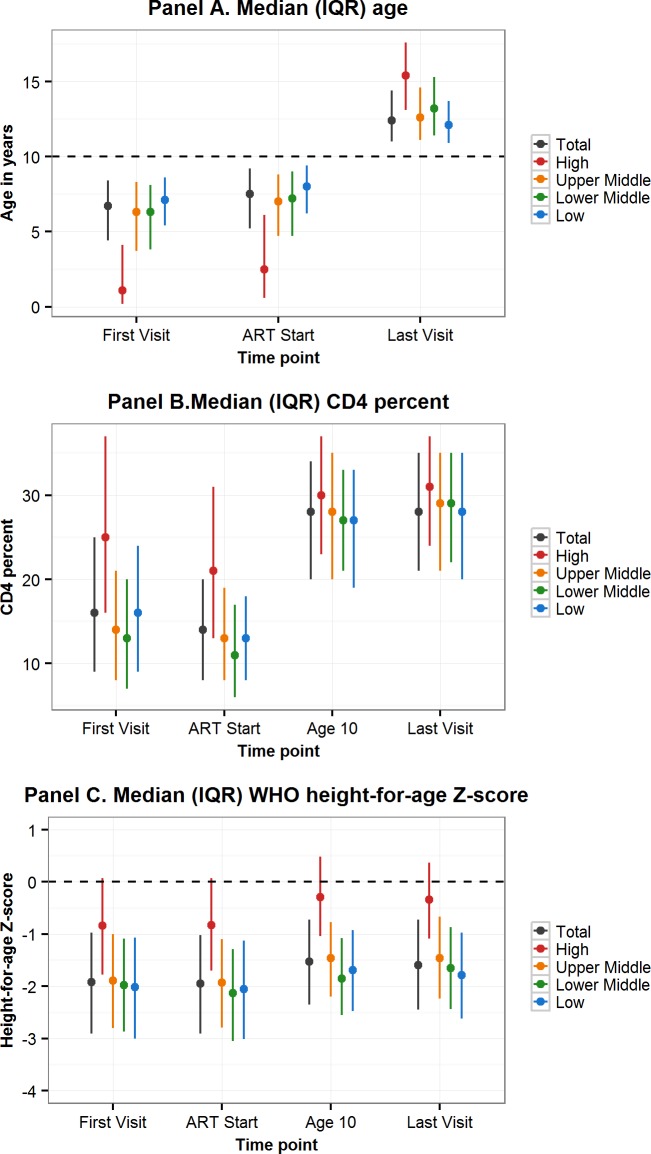
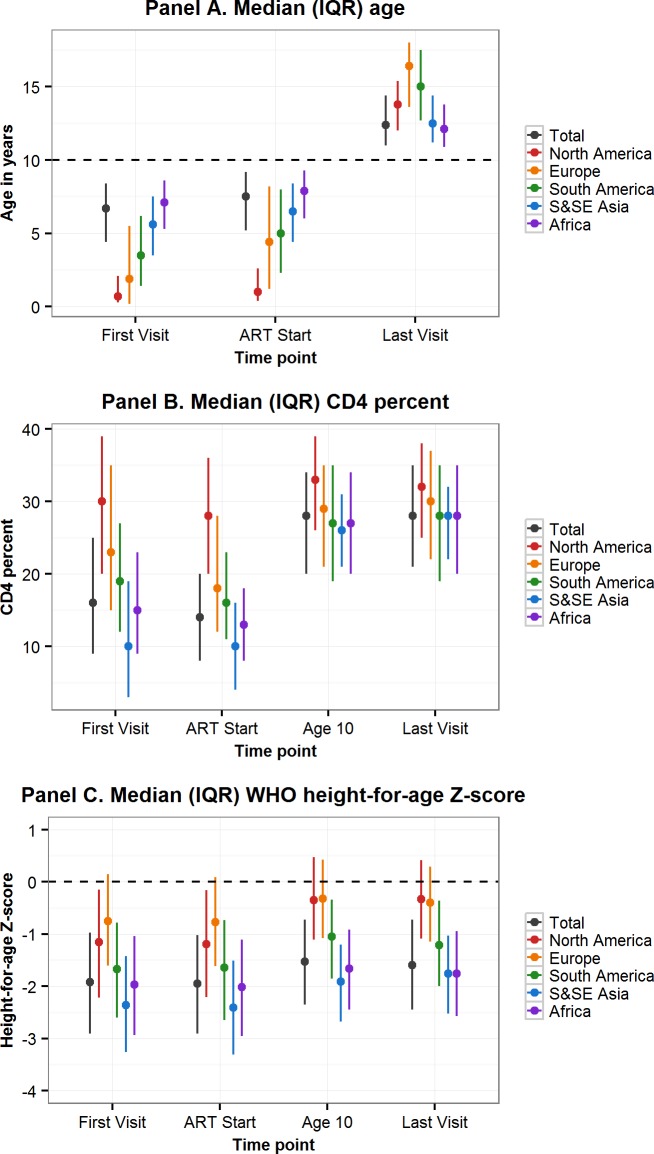
Through the Collaborative Initiative for Paediatric HIV Education and Research (CIPHER), individual retrospective longitudinal data from 12 cohort networks were pooled. All children infected with HIV who entered care before age 10 years, were not known to have horizontally acquired HIV, and were followed up beyond age 10 years were included in this analysis conducted from May 2016 to January 2017. Our primary analysis describes patient and treatment characteristics of APHs at key time points, including first HIV-associated clinic visit, antiretroviral therapy (ART) start, age 10 years, and last visit, and compares these characteristics by geographic region, country income group (CIG), and birth period. Our secondary analysis describes mortality, transfer out, and lost to follow-up (LTFU) as outcomes at age 15 years, using competing risk analysis. Among the 38,187 APHs included, 51% were female, 79% were from sub-Saharan Africa and 65% lived in low-income countries. APHs from 51 countries were included (Europe: 14 countries and 3,054 APHs; North America: 1 country and 1,032 APHs; South America and the Caribbean: 4 countries and 903 APHs; South and Southeast Asia: 7 countries and 2,902 APHs; sub-Saharan Africa, 25 countries and 30,296 APHs). Observation started as early as 1982 in Europe and 1996 in sub-Saharan Africa, and continued until at least 2014 in all regions. The median (interquartile range [IQR]) duration of adolescent follow-up was 3.1 (1.5-5.2) years for the total cohort and 6.4 (3.6-8.0) years in Europe, 3.7 (2.0-5.4) years in North America, 2.5 (1.2-4.4) years in South and Southeast Asia, 5.0 (2.7-7.5) years in South America and the Caribbean, and 2.1 (0.9-3.8) years in sub-Saharan Africa. Median (IQR) age at first visit differed substantially by region, ranging from 0.7 (0.3-2.1) years in North America to 7.1 (5.3-8.6) years in sub-Saharan Africa. The median age at ART start varied from 0.9 (0.4-2.6) years in North America to 7.9 (6.0-9.3) years in sub-Saharan Africa. The cumulative incidence estimates (95% confidence interval [CI]) at age 15 years for mortality, transfers out, and LTFU for all APHs were 2.6% (2.4%-2.8%), 15.6% (15.1%-16.0%), and 11.3% (10.9%-11.8%), respectively. Mortality was lowest in Europe (0.8% [0.5%-1.1%]) and highest in South America and the Caribbean (4.4% [3.1%-6.1%]). However, LTFU was lowest in South America and the Caribbean (4.8% [3.4%-6.7%]) and highest in sub-Saharan Africa (13.2% [12.6%-13.7%]). Study limitations include the high LTFU rate in sub-Saharan Africa, which could have affected the comparison of mortality across regions; inclusion of data only for APHs receiving ART from some countries; and unavailability of data from high-burden countries such as Nigeria.
To our knowledge, our study represents the largest multiregional epidemiological analysis of APHs. Despite probable under-ascertained mortality, mortality in APHs remains substantially higher in sub-Saharan Africa, South and Southeast Asia, and South America and the Caribbean than in Europe. Collaborations such as CIPHER enable us to monitor current global temporal trends in outcomes over time to inform appropriate policy responses.
在全球范围内,感染艾滋病毒的青少年人数持续增加。在这项研究中,我们汇集了观察性儿科艾滋病毒队列和队列网络的数据,允许在多个地区的“真实”环境中对感染艾滋病毒的青少年进行比较。我们描述了包括南美洲和加勒比地区、北美、欧洲、撒哈拉以南非洲以及南亚和东南亚在内的多个地区感染艾滋病毒的青少年的地理和时间特征以及死亡率结局。
通过儿童艾滋病毒教育和研究合作倡议(CIPHER),我们汇集了 12 个队列网络的个体回顾性纵向数据。本分析纳入了所有在 10 岁前感染艾滋病毒、未被发现通过水平途径感染艾滋病毒且在 10 岁后接受随访的儿童。本分析于 2016 年 5 月至 2017 年 1 月进行。我们的主要分析描述了感染艾滋病毒的青少年在关键时间点的患者和治疗特征,包括首次艾滋病毒相关临床就诊、开始抗逆转录病毒治疗(ART)、10 岁和最后一次就诊,并按地理位置、国家收入组(CIG)和出生时期进行比较。我们的次要分析描述了在 15 岁时的死亡率、转出和失访(LTFU)作为结局,使用竞争风险分析。在 38187 名感染艾滋病毒的青少年中,51%为女性,79%来自撒哈拉以南非洲,65%生活在低收入国家。来自 51 个国家的青少年被纳入分析(欧洲:14 个国家和 3054 名感染艾滋病毒的青少年;北美:1 个国家和 1032 名感染艾滋病毒的青少年;南美洲和加勒比地区:4 个国家和 903 名感染艾滋病毒的青少年;南亚和东南亚:7 个国家和 2902 名感染艾滋病毒的青少年;撒哈拉以南非洲:25 个国家和 30296 名感染艾滋病毒的青少年)。观察开始于欧洲的 1982 年和撒哈拉以南非洲的 1996 年,并在所有地区至少持续到 2014 年。在整个队列中,青少年随访的中位(四分位间距[IQR])持续时间为 3.1(1.5-5.2)年,在欧洲为 6.4(3.6-8.0)年,在北美为 3.7(2.0-5.4)年,在南亚和东南亚为 2.5(1.2-4.4)年,在南美洲和加勒比地区为 5.0(2.7-7.5)年,在撒哈拉以南非洲为 2.1(0.9-3.8)年。首次就诊的中位(IQR)年龄因地区而异,从北美 0.7(0.3-2.1)岁到撒哈拉以南非洲 7.1(5.3-8.6)岁不等。开始 ART 的中位年龄从北美 0.9(0.4-2.6)岁到撒哈拉以南非洲 7.9(6.0-9.3)岁不等。所有感染艾滋病毒的青少年在 15 岁时的死亡率、转出和失访的累积发生率估计值(95%置信区间[CI])分别为 2.6%(2.4%-2.8%)、15.6%(15.1%-16.0%)和 11.3%(10.9%-11.8%)。死亡率最低的是欧洲(0.8%[0.5%-1.1%]),最高的是南美洲和加勒比地区(4.4%[3.1%-6.1%])。然而,失访率最低的是南美洲和加勒比地区(4.8%[3.4%-6.7%]),最高的是撒哈拉以南非洲(13.2%[12.6%-13.7%])。研究的局限性包括撒哈拉以南非洲的高失访率,这可能影响了死亡率在各地区的比较;仅纳入了一些国家接受抗逆转录病毒治疗的感染艾滋病毒的青少年的数据;以及没有来自高负担国家(如尼日利亚)的数据。
据我们所知,我们的研究代表了最大的感染艾滋病毒的青少年多区域流行病学分析。尽管可能低估了死亡率,但撒哈拉以南非洲、南亚和东南亚以及南美洲和加勒比地区的感染艾滋病毒的青少年的死亡率仍然明显高于欧洲。像 CIPHER 这样的合作使我们能够监测全球范围内随着时间的推移,了解当前的全球时间趋势,以便为适当的政策应对提供信息。