Emerg Infect Dis. 2020 May;26(5):833-840. doi: 10.3201/eid2605.181746.
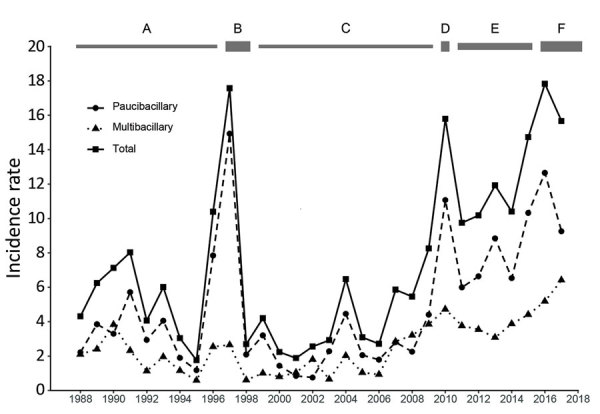
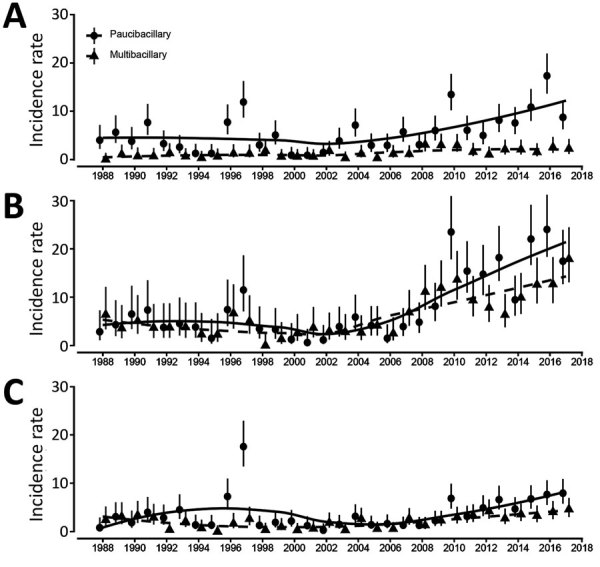
In Kiribati, unlike most countries, high and increasing numbers of cases of leprosy have been reported despite the availability of multidrug therapy and efforts to improve case finding and management. Historic records show that 28 cases had been identified by 1925. A systematic population survey in 1997 identified 135 new cases; the mean incidence rate for 1993-1997 was 7.4/10,000 population. After administering mass chemoprophylaxis, the country reached the elimination threshold (prevalence <1/10,000), but case numbers have rebounded. The mean annualized rate of new cases in 2013-2017 was 15/10,000 population, with the highest new case rates (>20/10,000 population) in the main population centers of South Tarawa and Betio. Spread is expected to continue in areas where crowding and poor socioeconomic conditions persist and may accelerate as sea levels rise from climate change. New initiatives to improve social conditions are needed, and efforts such as postexposure chemoprophylaxis should be implemented to prevent spread.
在基里巴斯,与大多数国家不同,尽管提供了多种药物治疗,并努力提高病例发现和管理水平,但仍报告了大量不断增加的麻风病病例。历史记录显示,到 1925 年已发现 28 例病例。1997 年的一次系统人口调查发现了 135 例新病例;1993-1997 年的平均发病率为 7.4/10,000 人口。在进行大规模化学预防之后,该国达到了消除阈值(流行率<1/10,000),但病例数量有所反弹。2013-2017 年新病例的平均年化率为 15/10,000 人口,在南塔拉瓦和贝蒂奥等主要人口中心的新病例率最高(>20/10,000 人口)。预计在拥挤和社会经济条件较差的地区仍将继续传播,并且随着气候变化导致海平面上升,传播速度可能会加快。需要采取新的措施来改善社会条件,并应实施接触后化学预防等措施,以防止传播。