School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina.
Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina.
Cancer. 2020 Jul 1;126(13):3084-3093. doi: 10.1002/cncr.32898. Epub 2020 Apr 21.
The National Cancer Institute's Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events, collected alongside the clinician-reported Common Terminology Criteria for Adverse Events, enables comparisons of patient and clinician reports on treatment toxicity.
In a multisite study of women receiving chemotherapy for early-stage breast cancer, symptom reports were collected on the same day from patients and their clinicians for 17 symptoms; their data were not shared with each other. The proportions of moderate, severe, or very severe patient-reported symptom severity were compared with the proportions of clinician-rated grade 2, 3, or 4 toxicity. Patient-clinician agreement was assessed via κ statistics. Chi-square tests investigated whether patient characteristics were associated with patient-clinician agreement.
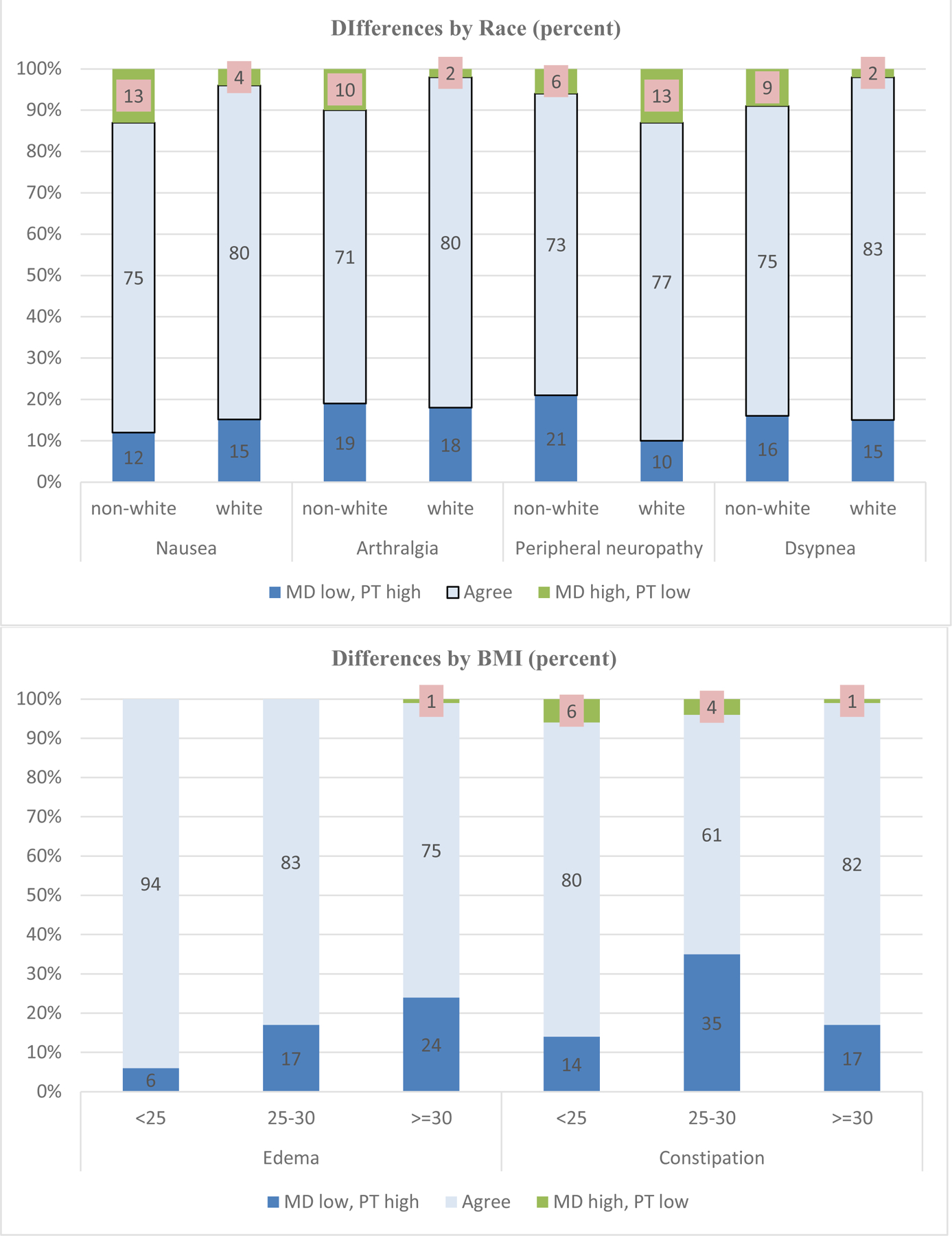
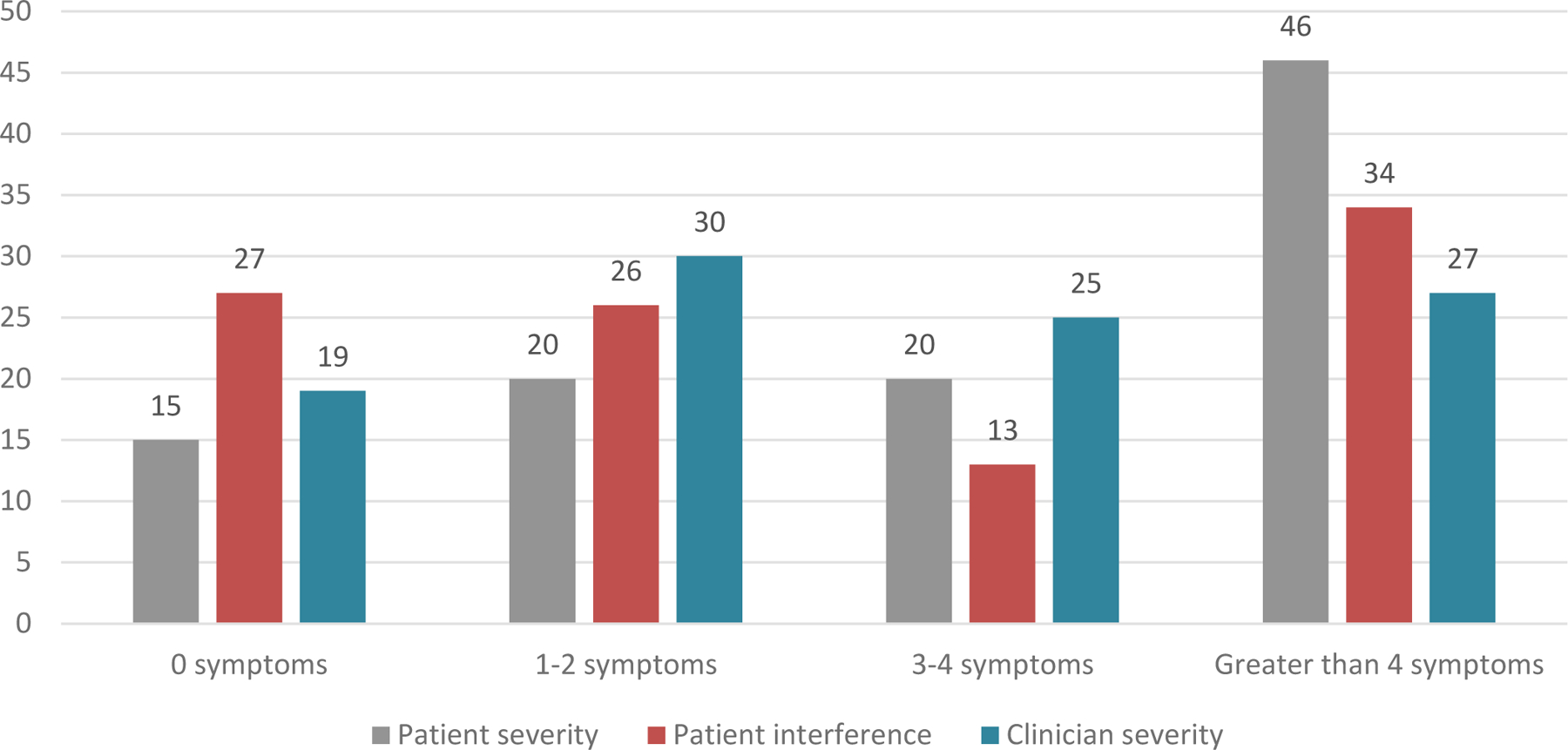
Among 267 women, the median age was 58 years (range, 24-83 years), and 26% were nonwhite. There was moderate scoring agreement (κ = 0.413-0.570) for 53% of symptoms, fair agreement for 41% (κ = 0.220-0.378), and slight agreement for 6% (κ = 0.188). For example, patient-reported and clinician-rated percentages were 22% and 8% for severe or very severe fatigue, 41% and 46% for moderate fatigue, 32% and 39% for mild fatigue, and 6% and 7% for none. Clinician severity scores were lower for nonwhite patients in comparison with white patients for peripheral neuropathy, nausea, arthralgia, and dyspnea.
Although clinician reporting of symptoms is common practice in oncology, there is suboptimal agreement with the gold standard of patient self-reporting. These data provide further evidence supporting the integration of patient-reported outcomes into oncological clinical research and clinical practice to improve monitoring of symptoms as well as timely interventions for symptoms.
美国国家癌症研究所的患者报告结局版通用不良事件术语标准,与临床医生报告的通用不良事件术语标准一起收集,使患者和临床医生对治疗毒性的报告能够进行比较。
在一项针对接受早期乳腺癌化疗的女性的多中心研究中,在同一天从患者及其临床医生那里收集了 17 种症状的报告;他们的数据彼此不共享。中度、重度或非常严重的患者报告症状严重程度的比例与临床医生评定的 2、3 或 4 级毒性的比例进行了比较。通过 κ 统计评估患者-临床医生一致性。卡方检验调查了患者特征是否与患者-临床医生一致性相关。
在 267 名女性中,中位年龄为 58 岁(范围,24-83 岁),26%是非裔美国人。对于 53%的症状,评分一致性为中度(κ=0.413-0.570),41%为适度(κ=0.220-0.378),6%为轻度(κ=0.188)。例如,患者报告的严重或非常严重疲劳的百分比和临床医生报告的百分比分别为 22%和 8%,中度疲劳的百分比分别为 41%和 46%,轻度疲劳的百分比分别为 32%和 39%,无疲劳的百分比分别为 6%和 7%。与白人患者相比,非裔美国患者的周围神经病变、恶心、关节痛和呼吸困难的临床医生严重程度评分较低。
尽管临床医生报告症状是肿瘤学的常见做法,但与患者自我报告的金标准存在不一致性。这些数据进一步支持将患者报告的结果纳入肿瘤学临床研究和临床实践中,以改善对症状的监测以及对症状的及时干预。