Beatson West of Scotland Cancer Centre, NHS Greater Glasgow & Clyde, Glasgow, UK.
Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow, UK.
Pharmacoepidemiol Drug Saf. 2020 Jun;29(6):653-663. doi: 10.1002/pds.4998. Epub 2020 Apr 21.
New treatments are introduced into standard care based on clinical trial results. However, it is not clear if these benefits are reflected in the broader population. This study analysed the clinical outcomes of patients with metastatic castration-resistant prostate cancer, treated with abiraterone and enzalutamide, within the Scottish National Health Service.
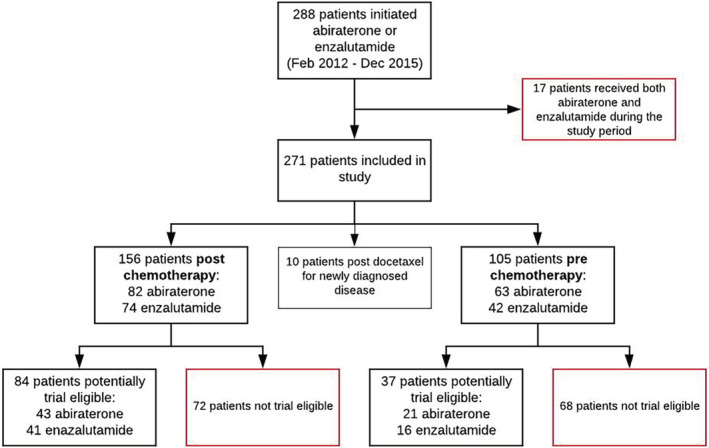
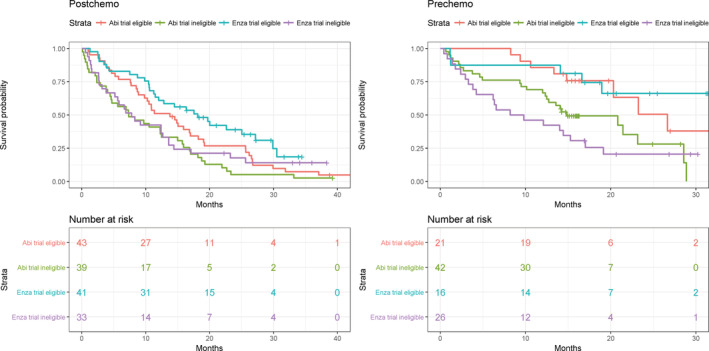
Retrospective cohort study using record linkage of routinely collected healthcare data (study period: February 2012 to February 2017). Overall survival (OS) was analysed using Kaplan-Meier methods and Cox Proportional Hazard models; a subgroup analysis comprised potentially trial-eligible patients.
Overall, 271 patients were included and 73.8% died during the study period. Median OS was poorer than in the pivotal trials, regardless of medication and indication: 10.8 months (95% confidence interval [CI] 8.6-15.1) and 20.9 months (95% CI 14.9-29.0) for abiraterone, and 12.6 months (95% CI 10.5-18.2) and 16.0 months (95% CI 9.8-not reached) for enzalutamide, post and pre chemotherapy, respectively. Only 46% of patients were potentially "trial eligible" and in this subgroup OS improved. Factors influencing survival included baseline performance status, and baseline prostate-specific antigen, alkaline phosphatase, and albumin levels.
Poorer prognostic features of non-trial eligible patients impact real-world outcomes of cancer medicines. Electronic record linkage of routinely collected healthcare data offers an opportunity to report outcomes on cancer medicines at scale and describe population demographics. The availability of such observational data to supplement clinical trial results enables patients and clinicians to make more informed treatment decisions, and policymakers to contextualise trial findings.
新的治疗方法基于临床试验结果被引入标准治疗方案中。然而,这些益处是否能在更广泛的人群中体现出来还不清楚。本研究分析了在苏格兰国家医疗服务体系中接受阿比特龙和恩扎卢胺治疗的转移性去势抵抗性前列腺癌患者的临床结局。
这是一项回顾性队列研究,使用常规收集的医疗保健数据进行记录链接(研究期间:2012 年 2 月至 2017 年 2 月)。使用 Kaplan-Meier 方法和 Cox 比例风险模型分析总生存期(OS);亚组分析包括可能有资格参加试验的患者。
共有 271 名患者入组,研究期间 73.8%的患者死亡。无论使用何种药物和适应症,中位 OS 均短于关键试验:阿比特龙的中位 OS 为 10.8 个月(95%置信区间 [CI] 8.6-15.1)和 20.9 个月(95% CI 14.9-29.0),恩扎卢胺的中位 OS 分别为 12.6 个月(95% CI 10.5-18.2)和 16.0 个月(95% CI 9.8-未达到),化疗前后。仅有 46%的患者有潜在的“试验资格”,且在这个亚组中 OS 有所改善。影响生存的因素包括基线体能状态以及基线前列腺特异性抗原、碱性磷酸酶和白蛋白水平。
非试验合格患者较差的预后特征影响癌症药物的实际疗效。常规收集医疗保健数据的电子记录链接提供了一个机会,可以大规模报告癌症药物的疗效,并描述人群特征。这种观察性数据的可用性可以补充临床试验结果,使患者和临床医生能够做出更明智的治疗决策,政策制定者可以使试验结果更具背景。