Hsieh Min-Shiau, Tong Shao-Syuan, Wei Bo-Chun, Chung Cheng-Chin, Cheng Yeung-Leung
Division of Thoracic Surgery, Department of Surgery, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, No. 289, Jian-Gao RD, Xindian District, New Taipei City, 23143, Taiwan.
School of Medicine, Tzu Chi University, Hualien, Taiwan.
J Cardiothorac Surg. 2020 Apr 21;15(1):65. doi: 10.1186/s13019-020-01106-1.
Pectus bar removal after Nuss repair is associated with the risk of major complications that are underreported. Of these, surgical bleeding is the main concern. Old age and placement of more than one bar are reported risk factors for pectus bar removal. In this study, we presented our experience regarding the modified skills required to minimize complications during bar removal, especially in adult patients.
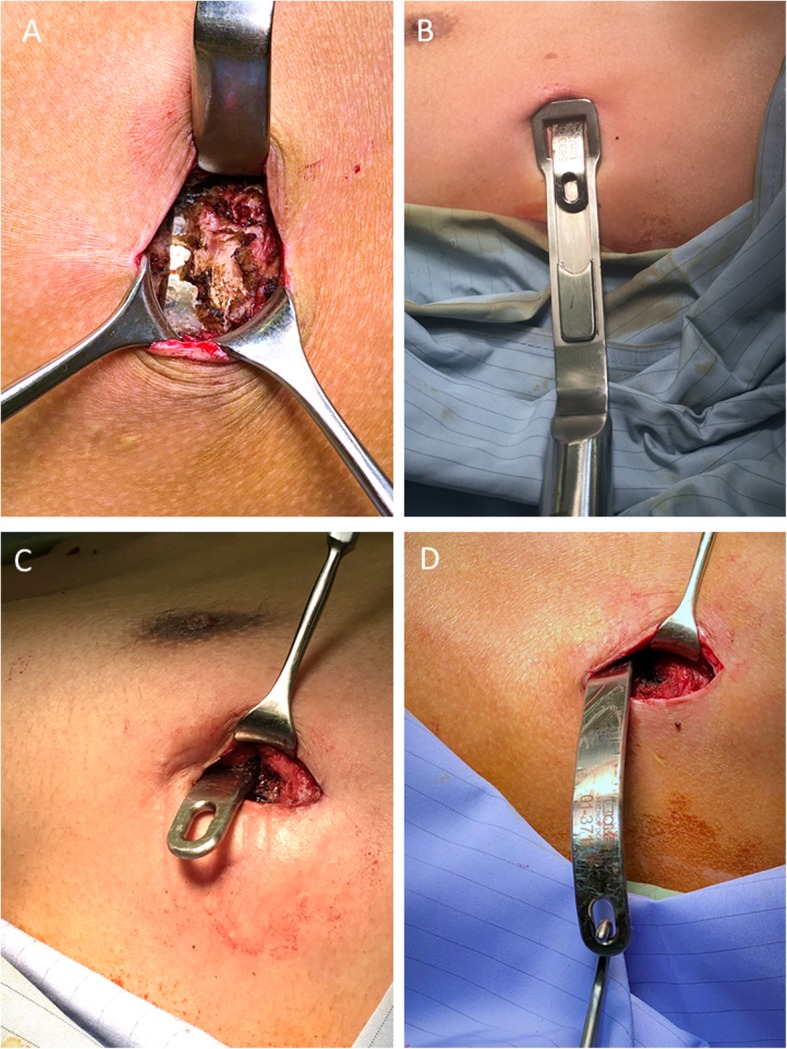
Consecutive patients who underwent pectus bar removal as the final stage of Nuss repair between August 2014 and December 2018 were included. The patients were positioned in the supine position. The bar(s) was (were) removed from the left side via the bilateral approach using the previous surgical scars after full dissection of the ends of the bar lateral to the hinge point and after straightening the right end of the bar. Bleeding was carefully checked after removal. An elastic bandage was wrapped around the chest after wound closure to prevent wound hematoma/seroma formation.
A total of 283 patients (260 male and 23 female), with a mean age of 22.8 ± 6.6 years at the time of the Nuss repair were included. The mean duration of pectus bar maintenance interval was 4.3 years (range: 1.9 to 9.8 years). A total of 200 patients (71%) had two bars. The mean estimated blood loss was 11.7 mL (range: 10 mL to 100 mL). Nine patients (3.1%) experienced complications, six had pneumothorax and three had wound hematoma. No major bleeding occurred. Adults and the use of more than one bar were not associated with a significantly higher rate of complications (P = 0.400 and P = 0.260, respectively).
Adult patients and removal of multiple bars were not risk factors for complications in our cohort. Skill in preventing intraoperative mediastinal traction, carefully controlling bleeding, and reducing the effect of dead space around the wounds could minimize the risk of bleeding complications. A multicentric study or case accumulation is needed to further evaluate the risk factors of removal pectus bar(s).
努氏修复术后取出鸡胸钢板与一些未被充分报道的严重并发症风险相关。其中,手术出血是主要关注点。据报道,高龄和使用多根钢板是取出鸡胸钢板的风险因素。在本研究中,我们介绍了在取出钢板过程中,特别是在成年患者中,为尽量减少并发症所需的改良技术经验。
纳入2014年8月至2018年12月期间作为努氏修复最后阶段接受鸡胸钢板取出术的连续患者。患者取仰卧位。在充分解剖钢板铰链点外侧的两端并拉直钢板右端后,经双侧入路从左侧通过先前的手术瘢痕取出钢板。取出后仔细检查出血情况。伤口闭合后用弹性绷带包扎胸部以防止伤口血肿/血清肿形成。
共纳入283例患者(男性260例,女性23例),努氏修复时的平均年龄为22.8±6.6岁。鸡胸钢板维持间隔的平均时长为4.3年(范围:1.9至9.8年)。共有200例患者(占71%)使用了两根钢板。估计平均失血量为11.7毫升(范围:10毫升至100毫升)。9例患者(占3.1%)出现并发症,6例发生气胸,3例出现伤口血肿。未发生大出血。成人和使用多根钢板与并发症发生率显著升高无关(分别为P = 0.400和P = 0.260)。
在我们的队列中,成年患者和取出多根钢板并非并发症的风险因素。预防术中纵隔牵引、仔细控制出血以及减少伤口周围死腔影响的技术可将出血并发症风险降至最低。需要进行多中心研究或病例积累以进一步评估取出鸡胸钢板的风险因素。