Heydweiller Andreas C, König Tatjana T, Yavuz S Tolga, Schwind Martin, Oetzmann von Sochaczewski Christina, Rohleder Stephan
Sektion Kinderchirurgie der Klinik und Poliklinik für Allgemein‑, Viszeral‑, Thorax- und Gefäßchirurgie, Universitätsklinikum Bonn, Bonn, Deutschland.
Klinik und Poliklinik für Kinderchirurgie, Universitätsmedizin Mainz, Mainz, Deutschland.
Chirurgie (Heidelb). 2023 Sep;94(9):796-803. doi: 10.1007/s00104-023-01914-w. Epub 2023 Jun 23.
Metal bar removal after the Nuss repair procedure is prone to be cancelled in cases of operating time shortages due it being suitable to be postponed without harming patients. Consequently, planning operation times as exactly as possible could be one solution.
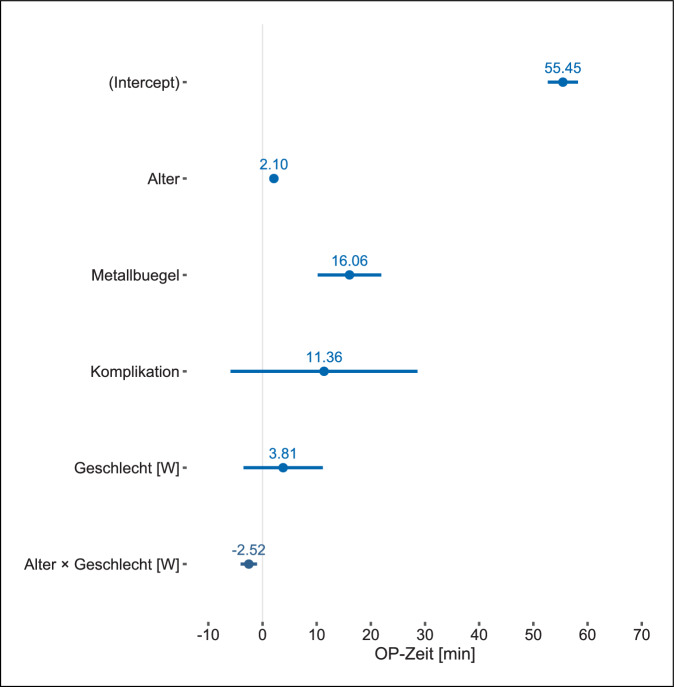
Statistical modelling of operation times of metal bar removal after Nuss repair using the prespecified independent predictors of age, sex, intraoperative complications, and number of implanted metal bars.
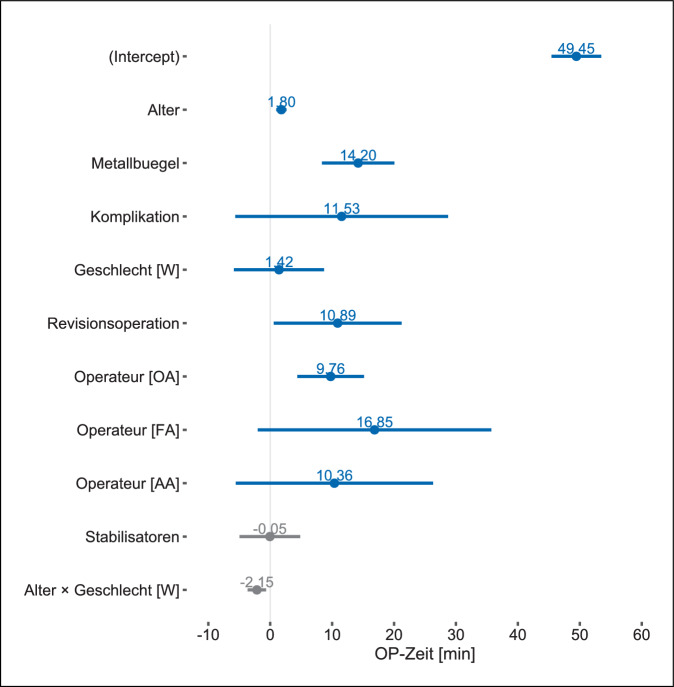
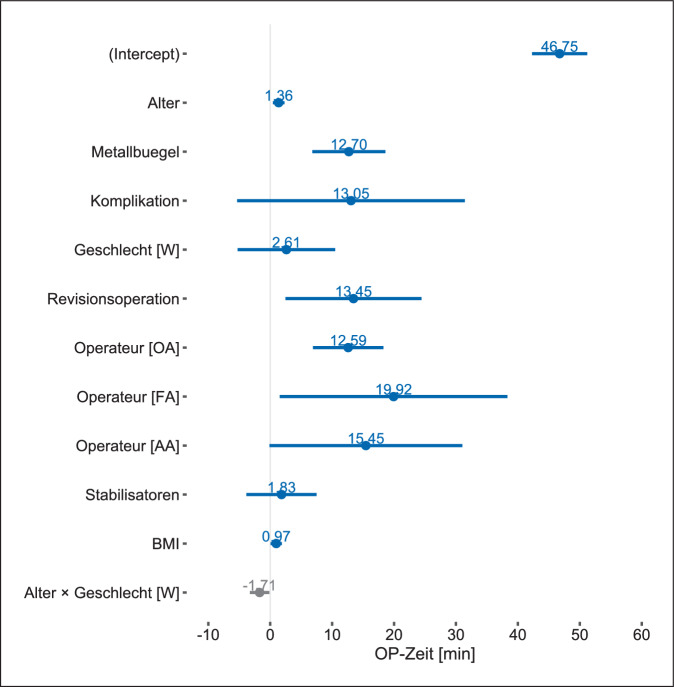
We included all patients whose operation notes included an operation time, which was modelled via linear regression and subject to internal validation via bootstrap. Exploratory analyses also consisted of the surgeon's experience, the number of stabilizers, the body mass index, and preceding re-do surgery for bar dislocation.
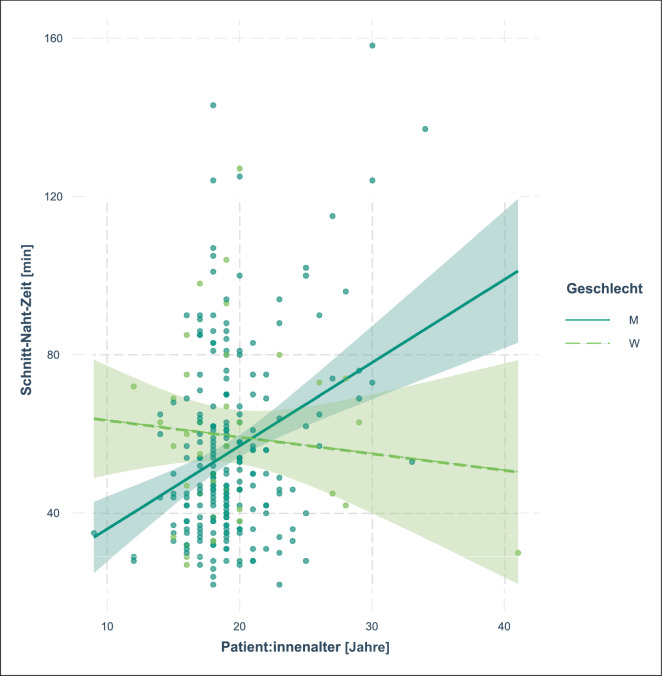
We included 265 patients (14% ♀) with a median age of 19 years (interquartile range 17-20 years), of whom 81% had 1 and 17% had 2 metal bars removed. The prespecified regression model was statistically significant (likelihood ratio 56; df = 5; P < 0.001) and had a bias corrected R of 0.148. Patient age influenced operation times by 2.1min per year of life (95% confidence interval 1.3-2.9min; P < 0.001) and 16min per explanted metal bar (95% confidence interval: 10-22min; P < 0.001).
The patient-specific factors of age and the number of explanted metal bars influenced the operation times and can be included into scheduling operation times.
在努氏修复手术后取出金属棒时,若手术时间不足,由于推迟取出对患者无害,该手术很可能被取消。因此,尽可能精确地规划手术时间可能是一种解决方案。
使用预先设定的年龄、性别、术中并发症及植入金属棒数量等独立预测因素,对努氏修复术后取出金属棒的手术时间进行统计建模。
我们纳入了所有手术记录中包含手术时间的患者,通过线性回归对手术时间进行建模,并通过自助法进行内部验证。探索性分析还包括外科医生的经验、稳定器数量、体重指数以及之前因金属棒移位进行的再次手术。
我们纳入了265例患者(14%为女性),中位年龄为19岁(四分位间距17 - 20岁),其中81%取出1根金属棒,17%取出2根金属棒。预先设定的回归模型具有统计学意义(似然比56;自由度 = 5;P < 0.001),偏差校正R为0.148。患者年龄对手术时间的影响为每年2.1分钟(95%置信区间1.3 - 2.9分钟;P < 0.001),每取出一根金属棒影响16分钟(95%置信区间:10 - 22分钟;P < 0.001)。
患者的年龄和取出的金属棒数量等特定因素会影响手术时间,可将其纳入手术时间安排。