Division of Surgery and Interventional Science, University College London, London, UK; Department of Urology, UCLH NHS Foundation Trust, London, UK.
Division of Surgery and Interventional Science, University College London, London, UK; Department of Radiology, UCLH NHS Foundation Trust, London, UK.
Eur Urol. 2020 Sep;78(3):443-451. doi: 10.1016/j.eururo.2020.03.035. Epub 2020 Apr 30.
Although the use of multiparametric magnetic resonance imaging (mpMRI) in active surveillance (AS) for prostate cancer is of increasing interest, existing data are derived from small cohorts.
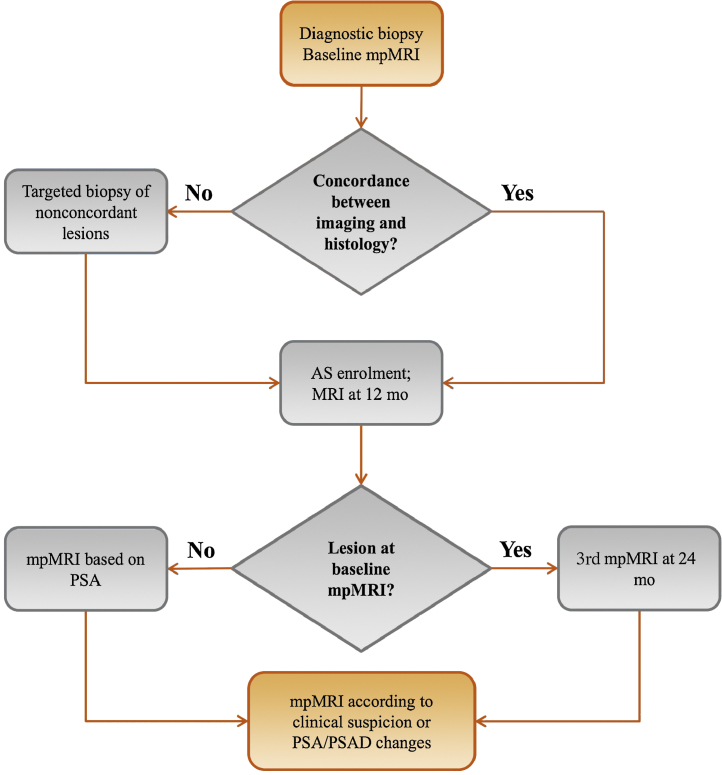
We describe clinical, histological, and radiological outcomes from an established AS programme, where protocol-based biopsies were omitted in favour of MRI-led monitoring.
DESIGN, SETTING, AND PARTICIPANTS: Data on 672 men enrolled in AS between August 2004 and November 2017 (inclusion criteria: Gleason 3 + 3 or 3 + 4 localised prostate cancer, presenting prostate-specific antigen <20 ng/ml, and baseline mpMRI) were collected from the University College London Hospital (UCLH) database.
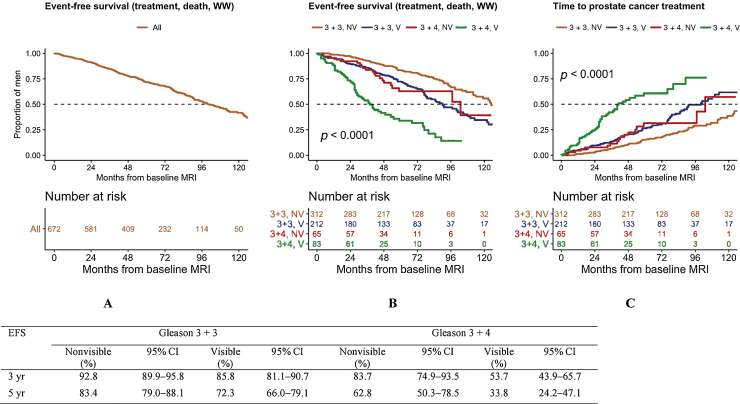
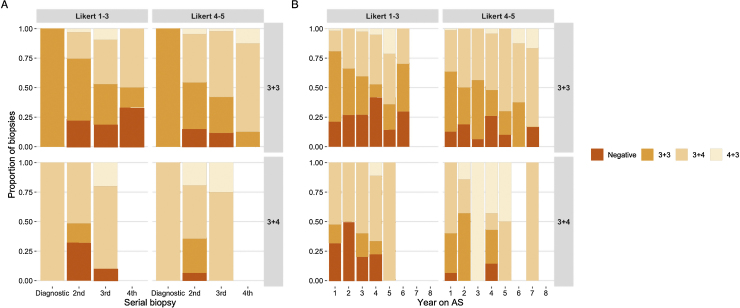
Primary outcomes were event-free survival (EFS; event defined as prostate cancer treatment, transition to watchful waiting, or death) and treatment-free survival (TFS). Secondary outcomes included rates of all-cause or prostate cancer-related mortality, metastasis, and upgrading to Gleason ≥4 + 3. Data on radiological and histological progression were also collected.
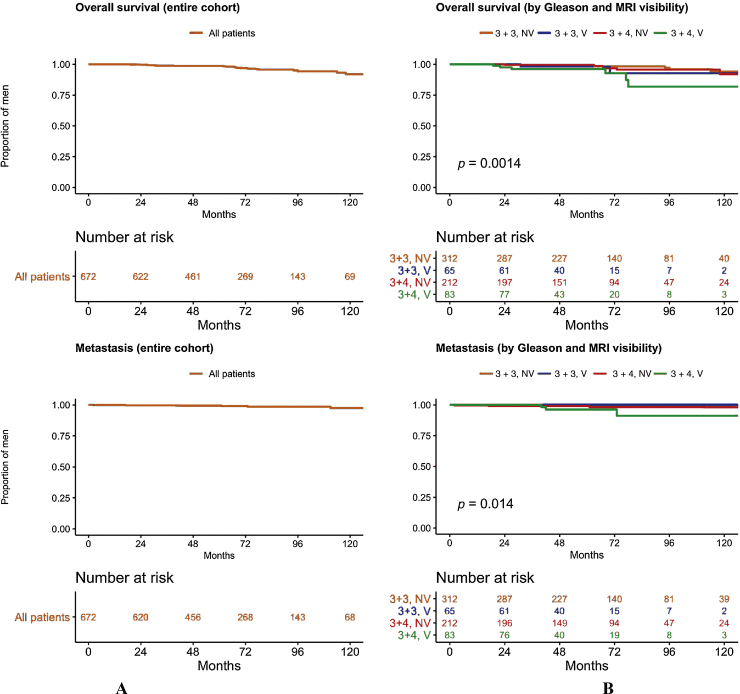
More than 3800 person-years (py) of follow-up were accrued (median: 58 mo; interquartile range 37-82 mo). Approximately 84.7% (95% confidence interval [CI]: 82.0-87.6) and 71.8% (95% CI: 68.2-75.6) of patients remained on AS at 3 and 5 yr, respectively. EFS and TFS were lower in those with MRI-visible (Likert 4-5) disease or secondary Gleason pattern 4 at baseline (log-rank test; p < 0.001). In total, 216 men were treated. There were 24 deaths, none of which was prostate cancer related (6.3/1000 py; 95% CI: 4.1-9.5). Metastases developed in eight men (2.1 events/1000 py; 95% CI: 1.0-4.3), whereas 27 men upgraded to Gleason ≥4 + 3 on follow-up biopsy (7.7 events/1000 py; 95% CI: 5.2-11.3).
The rates of discontinuation, mortality, and metastasis in MRI-led surveillance are comparable with those of standard AS. MRI-visible disease and/or secondary Gleason grade 4 at baseline are associated with a greater likelihood of moving to active treatment at 5 yr. Further research will concentrate on optimising imaging intervals according to baseline risk.
In this report, we looked at the outcomes of magnetic resonance imaging (MRI)-based surveillance for prostate cancer in a UK cohort. We found that this strategy could allow routine biopsies to be avoided. Secondary Gleason pattern 4 and MRI visibility are associated with increased rates of treatment. We conclude that MRI-based surveillance should be considered for the monitoring of small prostate tumours.
尽管多参数磁共振成像(mpMRI)在前列腺癌主动监测(AS)中的应用越来越受到关注,但现有数据来自于小队列。
我们描述了一个既定的 AS 项目的临床、组织学和影像学结果,该项目中,基于方案的活检被 MRI 引导的监测所取代。
设计、地点和参与者:数据来自于 2004 年 8 月至 2017 年 11 月间在伦敦大学学院医院(UCLH)数据库中入组的 672 名男性(纳入标准:Gleason 3+3 或 3+4 局限性前列腺癌,前列腺特异性抗原<20ng/ml,基线时行 mpMRI)。
主要结局为无事件生存(EFS;事件定义为前列腺癌治疗、转为观察等待或死亡)和治疗无失败生存(TFS)。次要结局包括全因或前列腺癌相关死亡率、转移和升级为 Gleason≥4+3 的发生率。还收集了影像学和组织学进展的数据。
共获得超过 3800 人年(中位数:58 个月;四分位间距 37-82 个月)的随访数据。大约 84.7%(95%置信区间 [CI]:82.0-87.6%)和 71.8%(95% CI:68.2-75.6%)的患者在 3 年和 5 年时仍在接受 AS。在基线时具有 MRI 可见(Likert 4-5)疾病或次要 Gleason 模式 4 的患者中,EFS 和 TFS 较低(对数秩检验;p<0.001)。共有 216 名男性接受了治疗。有 24 例死亡,均与前列腺癌无关(每 1000 人年 6.3 例;95% CI:4.1-9.5)。8 名男性发生转移(每 1000 人年 2.1 例;95% CI:1.0-4.3),而 27 名男性在随访活检中升级为 Gleason≥4+3(每 1000 人年 7.7 例;95% CI:5.2-11.3)。
MRI 引导监测的停药、死亡率和转移率与标准 AS 相当。基线时的 MRI 可见疾病和/或次要 Gleason 分级 4 与 5 年内更有可能转为积极治疗相关。进一步的研究将集中于根据基线风险优化影像学监测间隔。
在本报告中,我们研究了英国队列中基于 MRI 的前列腺癌监测的结果。我们发现,这种策略可以避免常规活检。次要 Gleason 模式 4 和 MRI 可见性与更高的治疗率相关。我们的结论是,基于 MRI 的监测应考虑用于小前列腺肿瘤的监测。