Shima Natsuki, Sawa Naoki, Yamanouchi Masayuki, Mizuno Hiroki, Kawada Masahiro, Sekine Akinari, Hiramatsu Rikako, Hayami Noriko, Hasegawa Eiko, Suwabe Tatsuya, Hoshino Junichi, Takaichi Kenmei, Ohashi Kenichi, Fujii Takeshi, Ubara Yoshifumi
Nephrology Center, Toranomon Hospital, 1-3-1, Takatsu, KajigayaKawasaki, Kanagawa, 212-0015, Japan.
Division of Rheumatology and Clinical Immunology, Department of Medicine, Jichi Medical University, Tochigi, Japan.
CEN Case Rep. 2020 Nov;9(4):338-343. doi: 10.1007/s13730-020-00483-9. Epub 2020 May 2.
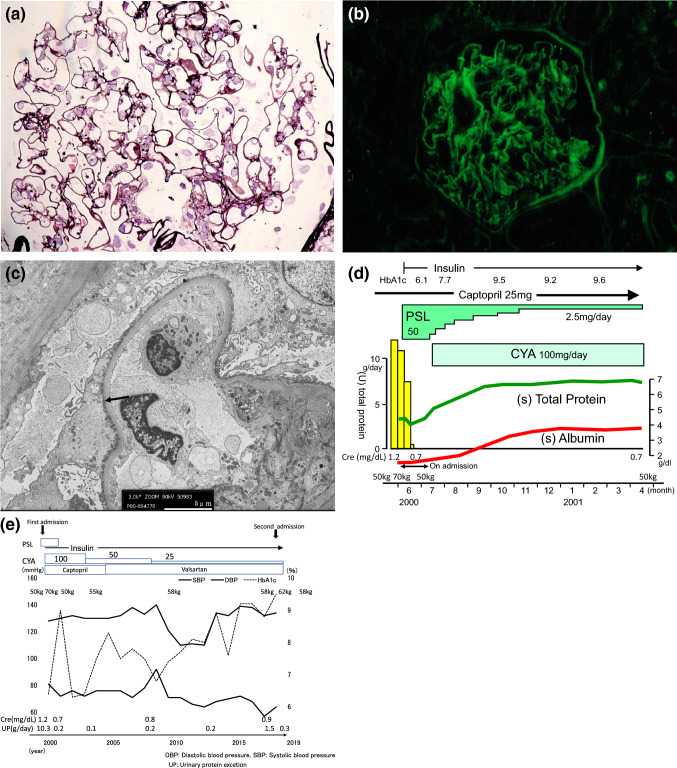
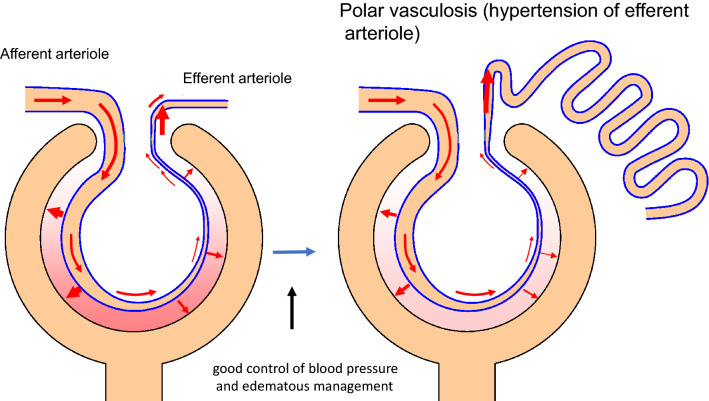
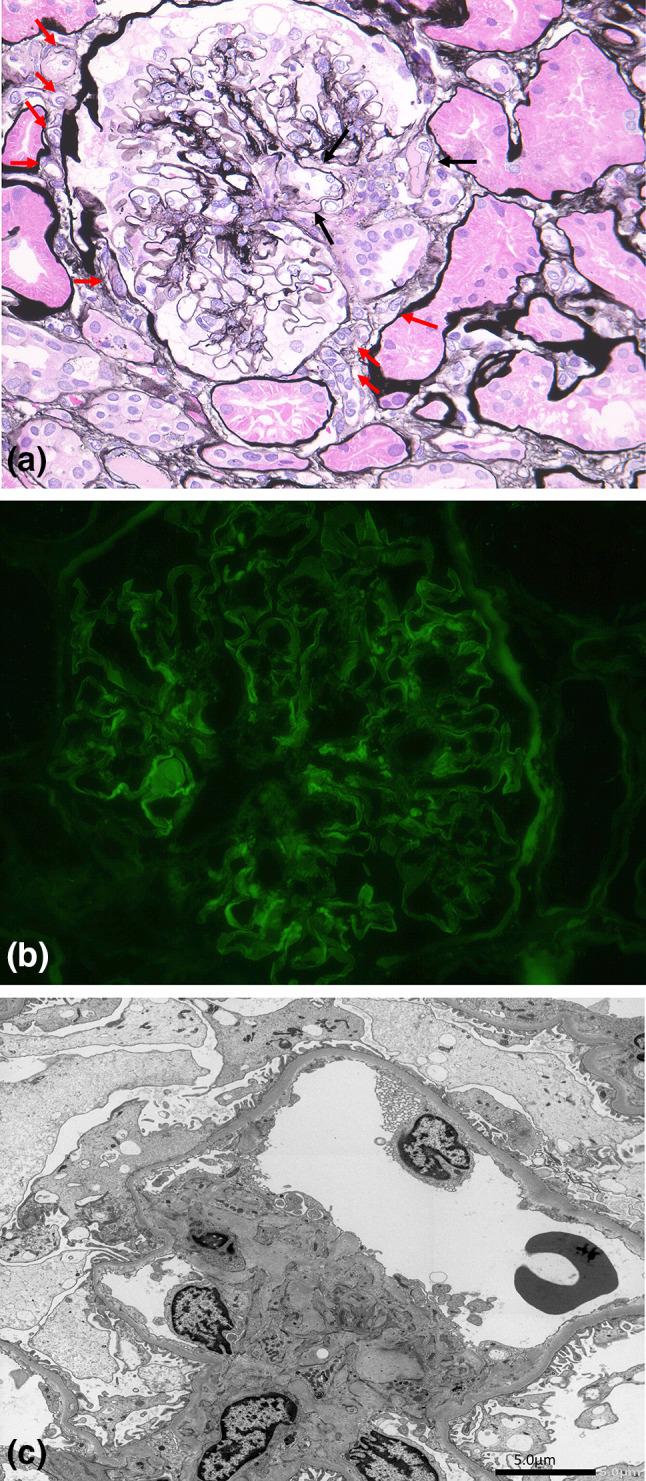
A renal histology of an 81-year-old man with a 30-year history of diabetes mellitus (DM), as well as diabetic retinopathy and neuropathy, was examined. The patient's blood pressure was controlled within the normal range (less than 140/75 mmHg) using antihypertensive agents including angiotensin receptor blocker. Edematous management was achieved by a strict salt diet (less than 6 g/per day). However, this patient's glycemic control was poor with HbA1c 8-10%. Serum creatinine was 0.87 mg/dL and estimated globular filtration rate (eGFR) was 64 ml/min/1.73m. Urinary protein excretion was 1.5 g/day. This patient's renal biopsy showed linear staining for IgG along the GBM by immunofluorescence microscopy, but light microscopy showed almost intact glomeruli, and the GBM was not thickened as revealed by electron microscopy with a width of 288-368 nm (< 430 nm). While arteriolar hyalinosis was severe, and polar vasculosis was observed around the glomerular vascular pole. This case indicates that long-standing hyperglycemia may induce polar vasculosis by the mechanism of angiogenesis, but diabetic glomerulopathy can become minor change, only when hypertension and edematous management could be controlled strictly.
对一名患有30年糖尿病史、糖尿病视网膜病变和神经病变的81岁男性进行了肾脏组织学检查。使用包括血管紧张素受体阻滞剂在内的抗高血压药物将患者血压控制在正常范围内(低于140/75 mmHg)。通过严格的低盐饮食(每天少于6克)实现水肿管理。然而,该患者血糖控制不佳,糖化血红蛋白(HbA1c)为8 - 10%。血清肌酐为0.87 mg/dL,估算肾小球滤过率(eGFR)为64 ml/min/1.73m²。尿蛋白排泄量为1.5 g/天。该患者的肾活检免疫荧光显微镜检查显示沿肾小球基底膜(GBM)有IgG线性染色,但光镜检查显示肾小球几乎完整,电镜检查显示GBM未增厚,宽度为288 - 368 nm(<430 nm)。虽然小动脉玻璃样变性严重,且在肾小球血管极周围观察到极周血管病。该病例表明,长期高血糖可能通过血管生成机制诱发极周血管病,但只有在严格控制高血压和水肿的情况下,糖尿病肾小球病才可能成为轻微病变。