Seong Jong-Mi, Shin Dongho, Sung Jae Woo, Cho Shinjay, Yang Jonghyup, Kang Sungmin, Moon Hyong Woo, Lee Kyu Won, Ha U-Syn
Ewha womans university, Department of pharmacy, Seoul, Republic of Korea.
Department of Urology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
J Cancer. 2020 Apr 6;11(14):4015-4022. doi: 10.7150/jca.38237. eCollection 2020.
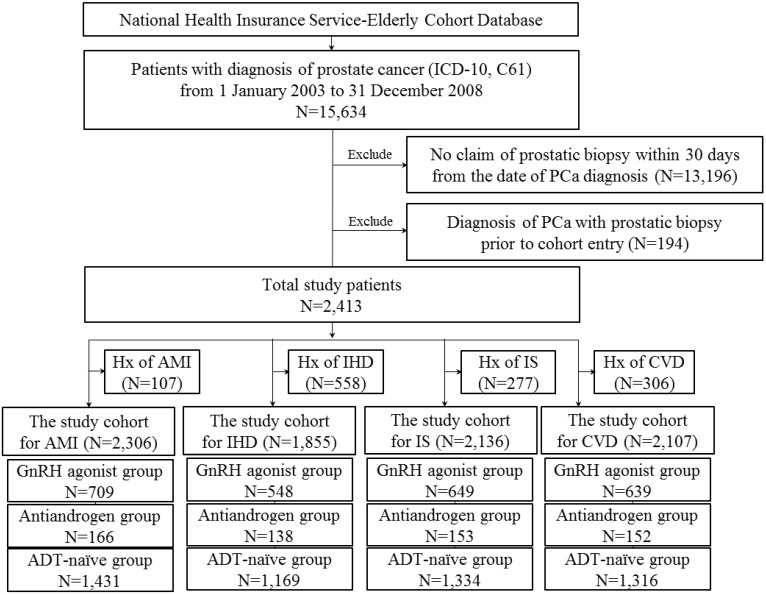
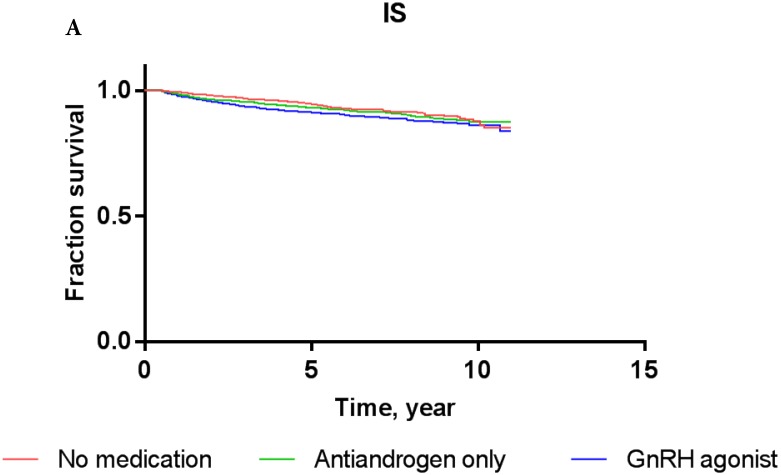
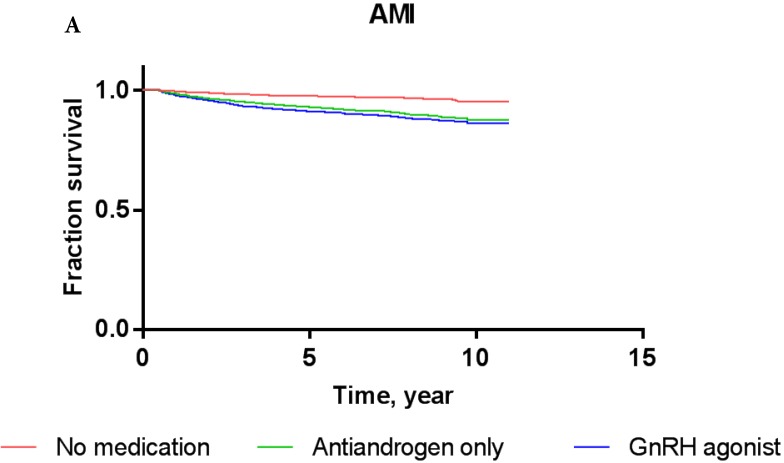
: To conduct a population-based study to determine whether the use of GnRH agonist and antiandrogens are associated with an increased risk of cardio-cerebrovascular disease (CCVD) in Asian patients with prostate cancer using the National Health Insurance Service-Elderly Cohort Database (NHIS-ECD). : We included a total of 2,413 men aged 60 years or older with prostate cancer between January 2003 and December 2008. Outcomes of interest included the first occurrence of cardiovascular events [acute myocardial infarction (AMI), ischemic heart disease (IHD)] and cerebrovascular events [ischemic stroke (IS), and cerebrovascular disease (CVD)]. : The 5-year AMI-free rates of patients diagnosed with prostate cancer and treated with GnRH agonists, antiandrogens alone, or androgen deprivation therapy (ADT)-naïve interventions were 97.0%, 96.5%, and 98.3%, respectively, while the 5-year IHD-free rates were 93.2%, 92.3%, and 94.5%, respectively. Exposure to GnRH agonists or antiandrogen regimens did not significantly increase the risk of AMI or IHD compared to ADT-naïve treatment in multivariate Cox proportional-hazards models after adjusting for other covariates. Five-year IS-free rates of patients exposed to GnRH agonists, antiandrogens alone, and those with ADT-naïve prostate cancer were 94.8%, 94.7%, and 95.5%, respectively, while the five-year CVD-free rates were 92.9%, 93.3%, and 94.6%, respectively. Cox proportional-hazards models also failed to show that men who received GnRH agonist or antiandrogen treatment alone carried a significantly increased risk for IS or CVD compared to ADT-naïve patients. : The current study based on Asian population suggests that treatment with neither GnRH agonist nor antiandrogens increases the risk of cardio-cerebrovascular disease compared to patients with ADT-naïve prostate cancer.
利用国民健康保险服务老年队列数据库(NHIS - ECD)开展一项基于人群的研究,以确定在亚洲前列腺癌患者中,使用促性腺激素释放激素(GnRH)激动剂和抗雄激素药物是否会增加心血管疾病(CCVD)的风险。我们纳入了2003年1月至2008年12月期间共2413名年龄在60岁及以上的前列腺癌男性患者。感兴趣的结局包括首次发生的心血管事件[急性心肌梗死(AMI)、缺血性心脏病(IHD)]和脑血管事件[缺血性中风(IS)和脑血管疾病(CVD)]。诊断为前列腺癌并接受GnRH激动剂、单独使用抗雄激素药物或未接受雄激素剥夺治疗(ADT)的初始干预措施的患者,其5年无AMI率分别为97.0%、96.5%和98.3%,而5年无IHD率分别为93.2%、92.3%和94.5%。在多变量Cox比例风险模型中,在调整其他协变量后,与未接受ADT的治疗相比,使用GnRH激动剂或抗雄激素治疗方案并未显著增加AMI或IHD的风险。接受GnRH激动剂、单独使用抗雄激素药物以及未接受ADT的前列腺癌患者的5年无IS率分别为94.8%、94.7%和95.5%,而5年无CVD率分别为92.9%、93.3%和94.6%。Cox比例风险模型也未能表明,与未接受ADT的患者相比,单独接受GnRH激动剂或抗雄激素治疗的男性发生IS或CVD的风险显著增加。基于亚洲人群的当前研究表明,与未接受ADT的前列腺癌患者相比,使用GnRH激动剂或抗雄激素药物治疗均不会增加心血管疾病的风险。