Department of General Practice and Elderly Care Medicine, University of Groningen, University Medical Center Groningen, PO Box 196, 9700 AD, Groningen, HPC FA21, the Netherlands.
Department of General Practice and Elderly Care Medicine, Amsterdam Public Health research institute, Amsterdam University Medical Centers, location VUmc, Amsterdam, the Netherlands.
BMC Geriatr. 2020 May 6;20(1):163. doi: 10.1186/s12877-020-01569-w.
Several efforts have been made to change management of neuropsychiatric symptoms (NPS) in nursing homes, however only few were successful. Numerous barriers to change in healthcare were identified, yet only one conceptual model is known to study their interrelationships. Unfortunately, this model does not discuss specific barriers encountered in nursing home practice. The aim of this study is to explore perceived barriers to change in the management of NPS in nursing homes and to construct a conceptual framework providing insight into the relative importance and interrelationships of these barriers when improving quality of care.
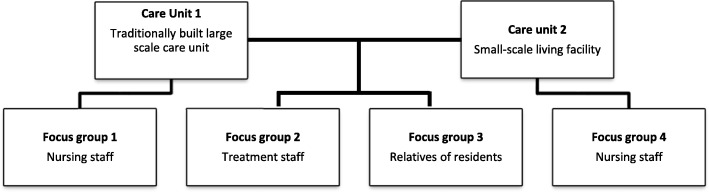
Four focus groups were conducted in different dementia special care units of one Dutch nursing home. Participants were either nursing staff, treatment staff or relatives of residents. Qualitative thematic analysis was conducted according to the five phases defined by Braun & Clarke. Finally, a conceptual framework showing the interrelations of barrier-themes was constructed using text fragments of the focus groups.
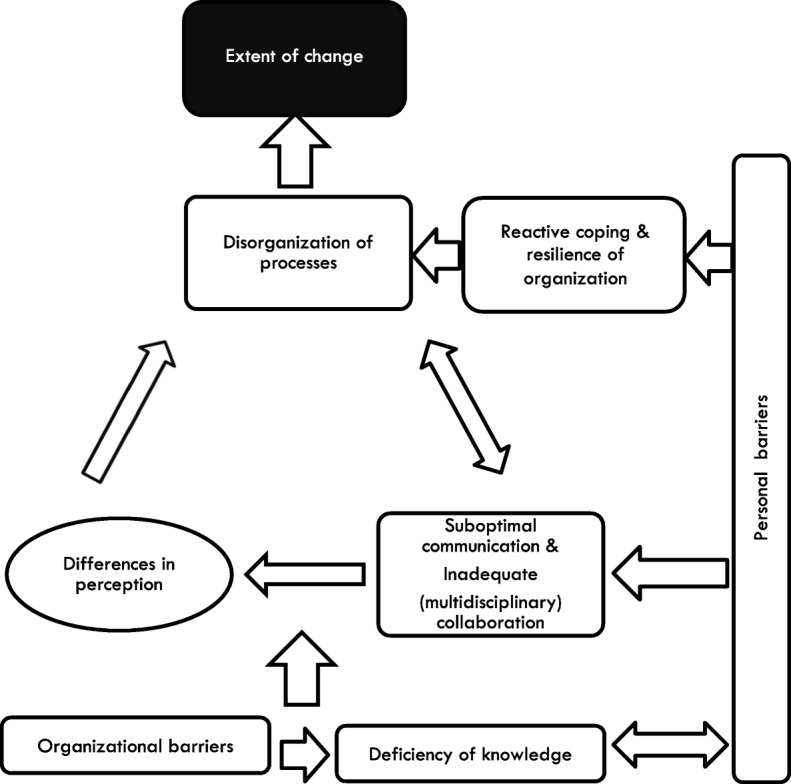
We constructed a conceptual framework consisting of eight themes of barriers explaining the extent to which change in NPS-management can be achieved: 'organizational barriers', 'personal barriers', 'deficiency of staff knowledge', 'suboptimal communication', 'inadequate (multidisciplinary) collaboration', 'disorganization of processes', 'reactive coping' and 'differences in perception'. Addressing 'organizational barriers' and 'deficiency of staff knowledge' is a precondition for change. 'Suboptimal communication' and 'inadequate (multidisciplinary) collaboration' play a key role in the extent of change achieved via the themes 'differences in perception' and 'disorganization of processes'. Furthermore, 'personal barriers' influence all themes - except 'organizational barriers' - and may cause 'reactive coping', which in turn may lead to 'difficulties to structure processes'.
A conceptual framework was created explaining the relationships between barriers towards achieving change focused on improving management of NPS in nursing homes. After this framework has been confirmed and refined in additional research, it can be used to study the interrelatedness of barriers to change, and to determine the importance of addressing them for achieving change in the provided care.
已经有多项努力致力于改变养老院的神经精神症状(NPS)管理,然而只有少数取得了成功。在医疗保健中发现了许多变革的障碍,但只有一个概念模型被用于研究它们之间的相互关系。不幸的是,这个模型并没有讨论在养老院实践中遇到的具体障碍。本研究旨在探讨改变养老院 NPS 管理中所面临的感知障碍,并构建一个概念框架,深入了解在提高护理质量时这些障碍的相对重要性和相互关系。
在一家荷兰养老院的不同痴呆症特别护理病房进行了四次焦点小组讨论。参与者要么是护理人员,要么是治疗人员,要么是居民的亲属。根据 Braun 和 Clarke 定义的五个阶段进行了定性主题分析。最后,使用焦点小组的文本片段构建了一个显示障碍主题相互关系的概念框架。
我们构建了一个概念框架,由八个障碍主题组成,解释了在多大程度上可以实现 NPS 管理的变革:“组织障碍”、“个人障碍”、“员工知识不足”、“沟通不佳”、“(多学科)合作不足”、“流程混乱”、“被动应对”和“感知差异”。解决“组织障碍”和“员工知识不足”是变革的前提。“沟通不佳”和“(多学科)合作不足”在通过“感知差异”和“流程混乱”实现的变革程度中起着关键作用。此外,“个人障碍”影响除“组织障碍”之外的所有主题,并可能导致“被动应对”,进而可能导致“难以组织流程”。
创建了一个解释实现改进养老院 NPS 管理变革目标的障碍之间关系的概念框架。在对该框架进行进一步研究并加以确认和完善之后,可用于研究变革障碍的相互关系,并确定为实现护理变革而解决这些障碍的重要性。