Medicine, University of California San Francisco, San Francisco, California, USA
Medicine, University of California San Francisco, San Francisco, California, USA.
Thorax. 2020 Aug;75(8):669-678. doi: 10.1136/thoraxjnl-2019-213988. Epub 2020 May 6.
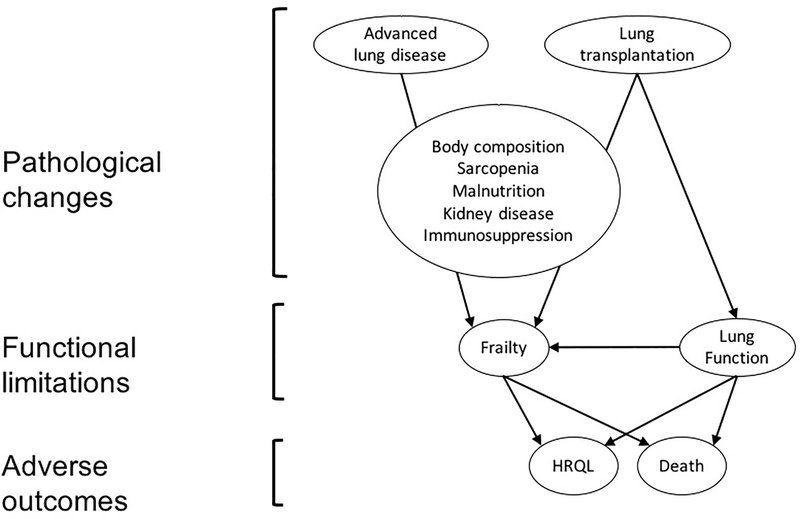
Lung transplantation and related medications are associated with pathobiological changes that can induce frailty, a state of decreased physiological reserve. Causes of persistent or emergent frailty after lung transplantation, and whether such transplant-related frailty is associated with key outcomes, are unknown.
Frailty and health-related quality of life (HRQL) were prospectively measured repeatedly for up to 3 years after lung transplantation. Frailty, quantified by the Short Physical Performance Battery (SPPB), was tested as a time-dependent binary and continuous predictor. The association of transplant-related frailty with HRQL and mortality was evaluated using mixed effects and Cox regression models, respectively, adjusting for age, sex, ethnicity, diagnosis, and for body mass index and lung function as time-dependent covariates. We tested the association between measures of body composition, malnutrition, renal dysfunction and immunosuppressants on the development of frailty using mixed effects models with time-dependent predictors and lagged frailty outcomes.
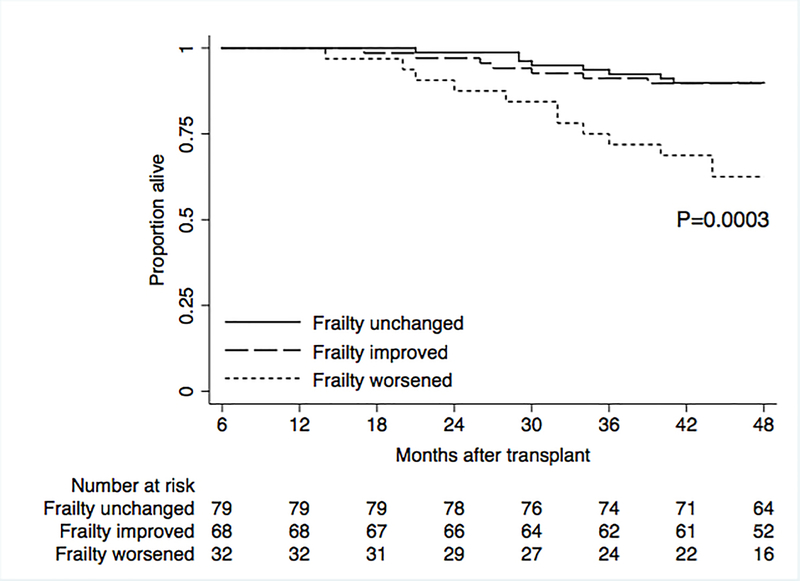
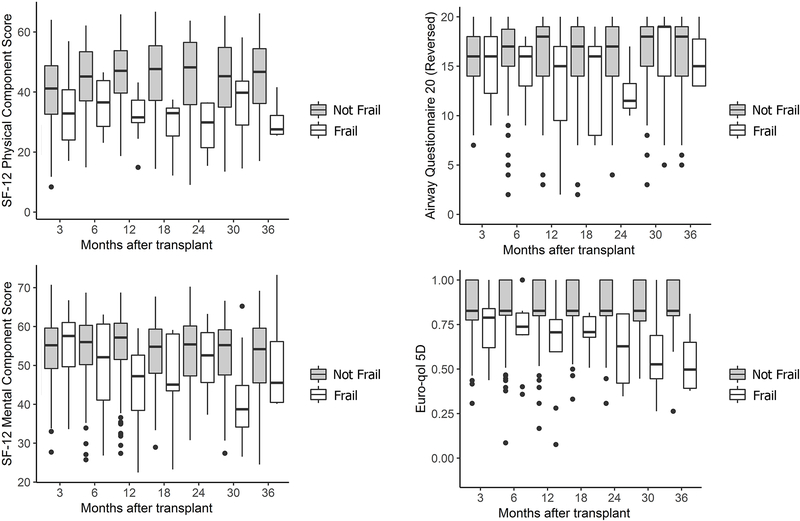
Among 259 adults (56% male; mean age 55.9±12.3 years), transplant-related frailty was associated with lower HRQL. Frailty was also associated with a 2.5-fold higher mortality risk (HR 2.51; 95% CI 1.21 to 5.23). Further, each 1-point worsening in SPPB was associated, on average, with a 13% higher mortality risk (HR 1.13; 95% CI 1.04 to 1.23). Secondarily, we found that sarcopenia, underweight and obesity, malnutrition, and renal dysfunction were associated with the development of frailty after transplant.
Transplant-related frailty is associated with lower HRQL and higher mortality in lung recipients. Abnormal body composition, malnutrition and renal dysfunction may contribute to the development of frailty after transplant. Confirming the role of these potential contributors and developing interventions to mitigate frailty may improve lung transplant success.
肺移植和相关药物治疗与可导致衰弱的病理生物学变化有关,衰弱是一种生理储备减少的状态。导致肺移植后持续或新出现衰弱的原因,以及这种与移植相关的衰弱是否与关键结局相关,目前尚不清楚。
在肺移植后长达 3 年内,前瞻性地多次重复测量衰弱和健康相关生活质量(HRQL)。通过短体适能表现测试(SPPB)量化的衰弱被作为一个时依性二分类和连续预测因素进行测试。使用混合效应和 Cox 回归模型分别评估移植相关衰弱与 HRQL 和死亡率的相关性,调整年龄、性别、种族、诊断以及体重指数和肺功能作为时依性协变量。我们使用具有时依性预测因素和滞后衰弱结局的混合效应模型,测试身体成分、营养不良、肾功能障碍和免疫抑制剂对衰弱发展的关联。
在 259 名成年人中(56%为男性;平均年龄 55.9±12.3 岁),与移植相关的衰弱与较低的 HRQL 相关。衰弱也与死亡率风险增加 2.5 倍相关(HR 2.51;95%CI 1.21 至 5.23)。此外,SPPB 每恶化 1 分,平均死亡率风险增加 13%(HR 1.13;95%CI 1.04 至 1.23)。其次,我们发现肌少症、体重不足和肥胖、营养不良和肾功能障碍与移植后衰弱的发展相关。
与移植相关的衰弱与肺移植受者较低的 HRQL 和较高的死亡率相关。异常的身体成分、营养不良和肾功能障碍可能导致移植后衰弱的发生。确认这些潜在因素的作用并开发减轻衰弱的干预措施可能会提高肺移植的成功率。