Centre for Mathematical Modelling of Infectious Diseases, Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine, Keppel Street, WC1E 7HT London, UK.
South African DSI-NRF Centre of Excellence in Epidemiological Modelling and Analysis (SACEMA), University of Stellenbosch, 19 Jonkershoek Road, Stellenbosch, 7600, South Africa.
J Travel Med. 2020 Aug 20;27(5). doi: 10.1093/jtm/taaa068.
We evaluated if interventions aimed at air travellers can delay local severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) community transmission in a previously unaffected country.
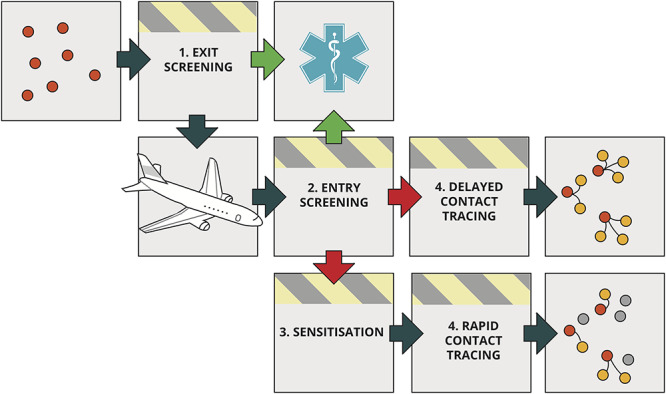
We simulated infected air travellers arriving into countries with no sustained SARS-CoV-2 transmission or other introduction routes from affected regions. We assessed the effectiveness of syndromic screening at departure and/or arrival and traveller sensitisation to the COVID-2019-like symptoms with the aim to trigger rapid self-isolation and reporting on symptom onset to enable contact tracing. We assumed that syndromic screening would reduce the number of infected arrivals and that traveller sensitisation reduces the average number of secondary cases. We use stochastic simulations to account for uncertainty in both arrival and secondary infections rates, and present sensitivity analyses on arrival rates of infected travellers and the effectiveness of traveller sensitisation. We report the median expected delay achievable in each scenario and an inner 50% interval.
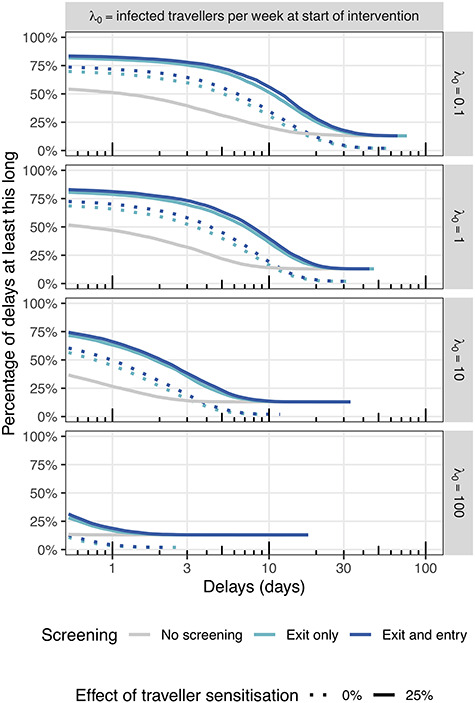
Under baseline assumptions, introducing exit and entry screening in combination with traveller sensitisation can delay a local SARS-CoV-2 outbreak by 8 days (50% interval: 3-14 days) when the rate of importation is 1 infected traveller per week at time of introduction. The additional benefit of entry screening is small if exit screening is effective: the combination of only exit screening and traveller sensitisation can delay an outbreak by 7 days (50% interval: 2-13 days). In the absence of screening, with less effective sensitisation, or a higher rate of importation, these delays shrink rapidly to <4 days.
Syndromic screening and traveller sensitisation in combination may have marginally delayed SARS-CoV-2 outbreaks in unaffected countries.
我们评估了针对航空旅行者的干预措施是否可以延迟先前未受影响的国家中本地严重急性呼吸系统综合征冠状病毒 2 型(SARS-CoV-2)的社区传播。
我们模拟了受感染的航空旅行者抵达没有持续 SARS-CoV-2 传播或来自受影响地区的其他传入途径的国家。我们评估了出发时和/或抵达时进行症状筛查以及对 COVID-19 样症状的旅行者敏感化的效果,目的是触发快速自我隔离并在出现症状时报告,以实现接触者追踪。我们假设症状筛查将减少感染入境者的数量,而旅行者敏感化将减少平均继发感染人数。我们使用随机模拟来考虑入境和继发感染率的不确定性,并对感染旅行者的入境率和旅行者敏感化的效果进行敏感性分析。我们报告每个方案可实现的中位数预期延迟时间以及内 50%间隔。
在基线假设下,当引入时每周有 1 名感染旅行者入境时,引入出口和入境筛查以及旅行者敏感化相结合可以将本地 SARS-CoV-2 暴发延迟 8 天(50%间隔:3-14 天)。如果出口筛查有效,则入境筛查的额外收益很小:仅出口筛查和旅行者敏感化的组合就可以将暴发延迟 7 天(50%间隔:2-13 天)。如果没有筛查,或者敏感化效果较差,或者入境率较高,则这些延迟会迅速缩小到<4 天。
症状筛查和旅行者敏感化的联合应用可能会略微延迟未受影响国家的 SARS-CoV-2 暴发。