Pediatric Intensive Care Unit, Soroka University Medical Center, Beer-Sheva, Israel; The Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel.
Pediatric Infectious Disease Unit, Soroka University Medical Center, Beer-Sheva, Israel; The Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel.
Pediatr Neonatol. 2020 Aug;61(4):406-413. doi: 10.1016/j.pedneo.2020.03.011. Epub 2020 Apr 10.
The purpose of this study was to determine factors characterizing children admitted to the Pediatric Intensive Care Unit (PICU) with community-acquired alveolar pneumonia (CAAP) to help clinicians assess disease severity upon initial assessment in the emergency department.
We prospectively collected demographic, clinical, and laboratory data of children <5 years with radiologically confirmed CAAP referred to the Soroka University Medical Center during 2001-2011. Three groups of children were compared: 1) those hospitalized in the PICU (PICU-CAAP); 2) those treated in the emergency department and discharged (ED-CAAP); and 3) those hospitalized in a pediatric ward (Hosp-CAAP).
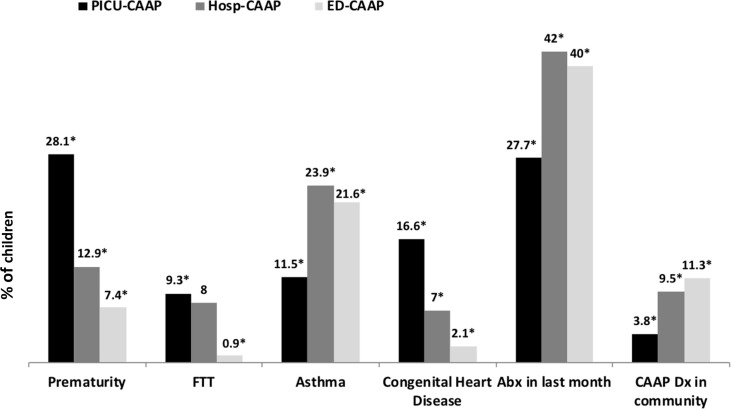
Of 9722 CAAP episodes, 367 (3.8%) were PICU-CAAP, 5552 (57.1%) Hosp-CAAP and 3803 (39.1%) ED-CAAP. In a univariate analysis, respiratory syncytial virus (RSV) was detected more commonly among PICU-CAAP than in Hosp-CAAP (P = 0.02) and ED-CAAP patients (P < 0.001). In a multivariate analysis, several factors were associated with PICU hospitalization versus ED-CAAP and Hosp-CAAP: Younger age (ORs: 1.04, [95%CI: 1.02-1.05] and 0.97 [0.96-0.98], respectively); prematurity (ORs: 2.16 [1.28-3.64] and 1.61 [1.15-2.26], respectively), lower O saturation (ORs: 1.32 [1.25-1.41] and 0.94[0.92-0.96]), higher respiratory rate (ORs: 1.06 [1.04-1.07] and 1.00 [1-1.01], respectively).
Children admitted to PICU were younger, had more respiratory syncytial virus (RSV) detection, were premature, had lower O saturation, and had a higher respiratory rate than those admitted to the general ward or those visiting the emergency department and subsequently discharged.
本研究旨在确定导致儿童因社区获得性肺泡肺炎(CAAP)入住儿科重症监护病房(PICU)的特征因素,以帮助临床医生在急诊科初步评估时评估疾病严重程度。
我们前瞻性地收集了 2001 年至 2011 年期间在索罗卡大学医学中心就诊的影像学确诊为 CAAP 的<5 岁儿童的人口统计学、临床和实验室数据。将患儿分为三组进行比较:1)入住 PICU 的患儿(PICU-CAAP);2)在急诊科接受治疗并出院的患儿(ED-CAAP);3)入住儿科病房的患儿(Hosp-CAAP)。
在 9722 例 CAAP 发作中,367 例(3.8%)为 PICU-CAAP,5552 例(57.1%)为 Hosp-CAAP,3803 例(39.1%)为 ED-CAAP。在单变量分析中,与 Hosp-CAAP 和 ED-CAAP 患儿相比,PICU-CAAP 患儿更常检测到呼吸道合胞病毒(RSV)(P=0.02 和 P<0.001)。多变量分析显示,与 ED-CAAP 和 Hosp-CAAP 相比,以下因素与 PICU 住院有关:年龄较小(ORs:1.04[95%CI:1.02-1.05]和 0.97[0.96-0.98]);早产(ORs:2.16[1.28-3.64]和 1.61[1.15-2.26])、较低的 O 饱和度(ORs:1.32[1.25-1.41]和 0.94[0.92-0.96])、较高的呼吸频率(ORs:1.06[1.04-1.07]和 1.00[1-1.01])。
与入住普通病房或急诊科后出院的患儿相比,入住 PICU 的患儿年龄较小,呼吸道合胞病毒(RSV)检测阳性率较高,早产儿比例较高,O 饱和度较低,呼吸频率较高。