Budhathoki Shyam Sundar, Sunny Avinash K, Paudel Pragya Gautam, Thapa Jeevan, Basnet Lila Bahadur, Karki Sandeepa, Gurung Rejina, Paudel Prajwal, Kc Ashish
Golden Community, Lalitpur, Nepal.
2Department of Primary Care and Public Health, School of Public Health, Imperial College London, London, UK.
Arch Public Health. 2020 May 7;78:39. doi: 10.1186/s13690-020-00424-z. eCollection 2020.
Every year, neonatal infections account for approximately 750,000 neonatal deaths globally. It is the third major cause of neonatal death, globally and in Nepal. There is a paucity of data on clinical aetiology and outcomes of neonatal infection in Nepal. This paper aims to assess the incidence and risk factors of neonatal infection in babies born in public hospitals of Nepal.
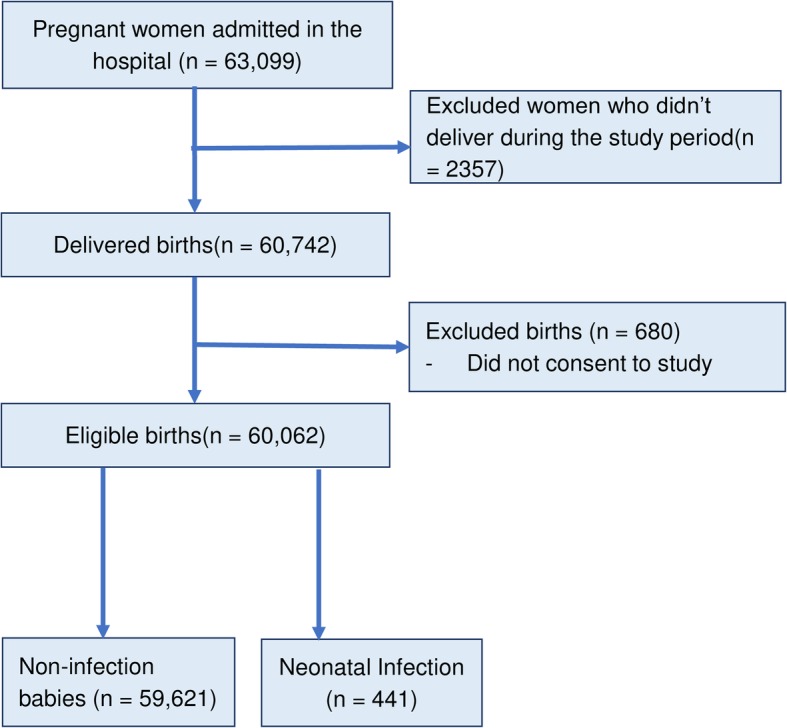
This is a prospective cohort study conducted for a period of 14 months, nested within a large-scale cluster randomized control trial which evaluated the Helping Babies Breathe Quality Improvement package in 12 public hospitals in Nepal. All the mothers who consented to participate within the study and delivered in these hospitals were included in the analysis. All neonates admitted into the sick newborn care unit weighing > 1500 g or/and 32 weeks or more gestation with clinical signs of infection or positive septic screening were taken as cases and those that did not have an infection were the comparison group. Bivariate and multi-variate analysis of socio-demographic, maternal, obstetric and neonatal characteristics of case and comparison group were conducted to assess risk factors associated with neonatal infection.
The overall incidence of neonatal infection was 7.3 per 1000 live births. Babies who were born to first time mothers were at 64% higher risk of having infection (aOR-1.64, 95% CI, 1.30-2.06, -value< 0.001). Babies born to mothers who had no antenatal check-up had more than three-fold risk of infection (aOR-3.45, 95% CI, 1.82-6.56, -value< 0.001). Babies born through caesarean section had more than two-fold risk (aOR-2.06, 95% CI, 1.48-2.87, -value< 0.001) and babies with birth asphyxia had more than three-fold risk for infection (aOR-3.51, 95% CI, 1.71-7.20, p-value = 0.001).
Antepartum factors, such as antenatal care attendance, and intrapartum factors such as mode of delivery and birth asphyxia, were risk factors for neonatal infections. These findings highlight the importance of ANC visits and the need for proper care during resuscitation in babies with birth asphyxia.
每年,全球约有75万例新生儿死亡是由新生儿感染所致。在全球及尼泊尔,这是新生儿死亡的第三大主要原因。尼泊尔关于新生儿感染的临床病因及转归的数据匮乏。本文旨在评估尼泊尔公立医院出生婴儿的新生儿感染发病率及危险因素。
这是一项为期14个月的前瞻性队列研究,嵌套于一项大规模整群随机对照试验中,该试验在尼泊尔的12家公立医院评估了“帮助婴儿呼吸质量改进包”。所有同意参与本研究并在这些医院分娩的母亲均纳入分析。所有入住患病新生儿护理单元、体重>1500克或/和孕周32周及以上且有感染临床体征或败血症筛查呈阳性的新生儿作为病例组,未感染的新生儿作为对照组。对病例组和对照组的社会人口学、母亲、产科及新生儿特征进行双变量和多变量分析,以评估与新生儿感染相关的危险因素。
新生儿感染的总体发病率为每1000例活产7.3例。初产妇所生婴儿感染风险高64%(调整后比值比[aOR]-1.64,95%置信区间[CI],1.30 - 2.06,P值<0.001)。未进行产前检查的母亲所生婴儿感染风险高出三倍多(aOR-3.45,95%CI,1.82 - 6.56,P值<0.001)。剖宫产出生的婴儿感染风险高出两倍多(aOR-2.06,95%CI,1.48 - 2.87,P值<0.001),出生时窒息的婴儿感染风险高出三倍多(aOR-3.51,95%CI,1.71 - 7.20,P值 = 0.001)。
产前因素,如产前检查次数,以及产时因素,如分娩方式和出生窒息,均为新生儿感染的危险因素。这些发现凸显了产前检查的重要性以及对出生窒息婴儿复苏时进行恰当护理的必要性。