Department of Neurology, University of Michigan, Ann Arbor.
Department of Neurology, Ann Arbor Veteran's Affairs, Ann Arbor, Michigan.
JAMA Netw Open. 2020 May 1;3(5):e204702. doi: 10.1001/jamanetworkopen.2020.4702.
Assessment of functional outcomes is currently limited by a lack of large data sets. Functional assessments are included in Medicare rehabilitation assessment files, yet the validity of these measures in routine care is unknown.
To evaluate the validity of individual-level routine care functional assessments in Medicare rehabilitation settings compared with criterion-standard National Health and Aging Trends Study (NHATS) research assessments obtained no more than 90 days later.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study of individuals aged 65 years and older used the 2011 to 2015 NHATS linked with Medicare assessment files. Individuals with a discharge assessment from inpatient rehabilitation facilities, skilled nursing facilities, or home health agencies and a criterion-standard NHATS assessment were included. Data analysis was performed June 2019 to November 2019.
Summary functional assessment based on independence with eating, toilet hygiene, bathing, dressing, transfers, and mobility or walking. Linear regression was used to assess agreement between the 2 scales, adjusting for time between assessments and rehabilitation setting.
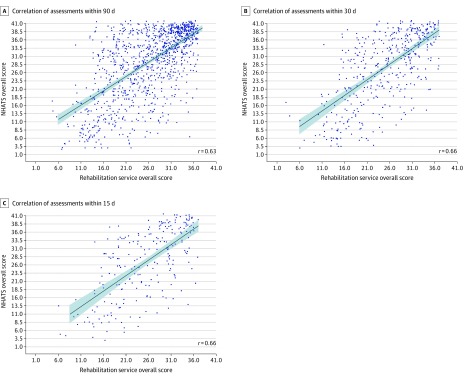
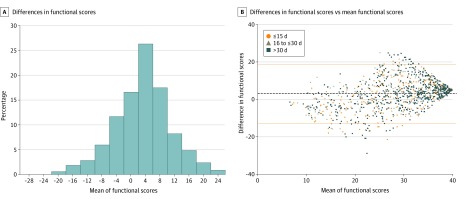
A total of 1036 adults aged 65 years and older (671 [64.8%] aged ≥80 years; 670 [64.7%] women; 685 [66.1%] white participants) met the study criteria. The correlation of the assessments was 0.63 (95% CI, 0.59 to 0.66; mean [SD] rehabilitation score, 27.5 [7.2]; mean [SD] NHATS score, 30.5 [10.1]). The correlation increased to 0.66 (95% CI, 0.60 to 0.71) for assessments no more than 30 days apart. The linear regression model adjusting for rehabilitation setting and days between evaluations found the assessments were strongly correlated (β = 1.00 [95% CI, 0.93 to 1.08]; intercept, 0.72 [95% CI, -1.79 to 3.24]; R2 = 0.42). Differences in scores were generally small (mean [SD] of NHATS - rehabilitation score, 2.96 [7.91]), and only 59 assessments (5.7%) differed by more than 2 SDs of the mean difference. Rehabilitation service scores were typically higher than NHATS scores in individuals with lower mean scores; however, the population with lower mean scores was small (156 [15.1%]).
In this large sample of older US adults, routine care rehabilitation facility functional assessments had overall moderate correlation with criterion-standard research assessments.
目前,功能评估受到缺乏大型数据集的限制。功能评估包含在医疗保险康复评估文件中,但这些措施在常规护理中的有效性尚不清楚。
评估医疗保险康复环境中常规护理个体功能评估的有效性,与随后不超过 90 天获得的标准标准国家健康与老龄化趋势研究(NHATS)研究评估进行比较。
设计、地点和参与者:本项横断面研究使用 2011 年至 2015 年 NHATS 与医疗保险评估文件进行关联,纳入年龄在 65 岁及以上的个体。纳入具有住院康复设施、熟练护理设施或家庭保健机构出院评估且具有标准 NHATS 评估的个体。数据分析于 2019 年 6 月至 2019 年 11 月进行。
基于进食、厕所卫生、洗澡、穿衣、转移和活动或行走独立性的综合功能评估。使用线性回归来评估两种量表之间的一致性,同时调整评估时间和康复环境的影响。
共有 1036 名年龄在 65 岁及以上的成年人(≥80 岁 671 人[64.8%];女性 670 人[64.7%];685 名白人参与者[66.1%])符合研究标准。评估的相关性为 0.63(95%置信区间,0.59 至 0.66;康复评分的平均值[标准差]为 27.5[7.2];NHATS 评分的平均值[标准差]为 30.5[10.1])。评估结果在间隔不超过 30 天的情况下增加到 0.66(95%置信区间,0.60 至 0.71)。调整康复环境和评估天数的线性回归模型发现评估结果具有很强的相关性(β=1.00[95%置信区间,0.93 至 1.08];截距,0.72[95%置信区间,-1.79 至 3.24];R2=0.42)。评分差异通常较小(NHATS-康复评分的平均值[标准差]为 2.96[7.91]),只有 59 次评估(5.7%)差异超过平均值差异的 2 个标准差。在平均得分较低的个体中,康复服务评分通常高于 NHATS 评分;然而,平均得分较低的人群较小(156[15.1%])。
在这项针对美国老年人群的大型研究中,常规护理康复设施的功能评估与标准研究评估总体上具有中度相关性。