Cancer Center, Massachusetts General Hospital, Boston, Massachusetts, USA.
Department of Medicine, Harvard Medical School, Boston, Massachusetts, USA.
J Immunother Cancer. 2020 May;8(1). doi: 10.1136/jitc-2019-000451.
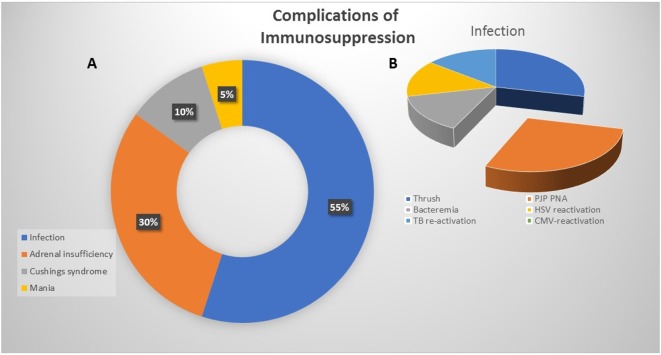
Immune-related colitis is a common, often serious complication of immune checkpoint inhibition (ICI). Although endoscopy is not strictly recommended for any grade of diarrhea/colitis, emerging evidence suggests that endoscopic evaluation may have important therapeutic implications. In this retrospective study, we sought to comprehensively characterize the clinical and histologic features of ICI-induced colitis with a specific focus on evaluating the prognostic role of endoscopy.
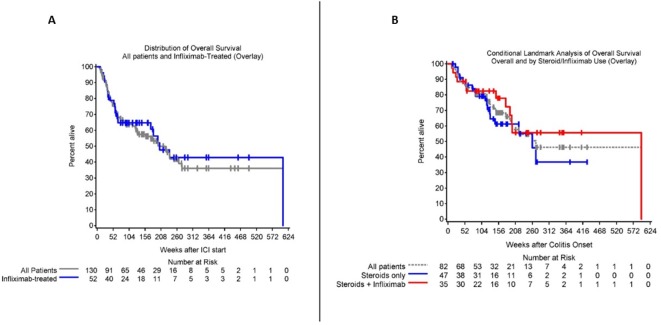
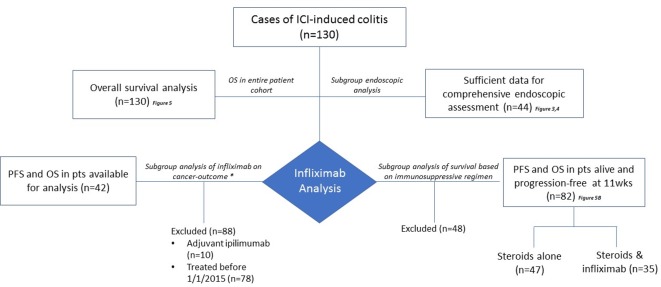
Data were collected from the medical records of 130 patients with confirmed ICI-induced colitis. In a subset of patients (n=44) with endoscopic and pathologic data, endoscopic data were scored using the Mayo Endoscopic Score (MES) with scores ranging from 0 (no inflammation) to 3 (colonic ulceration). The impact of infliximab on antitumor outcomes was evaluated using progression-free survival (PFS) and overall survival (OS).
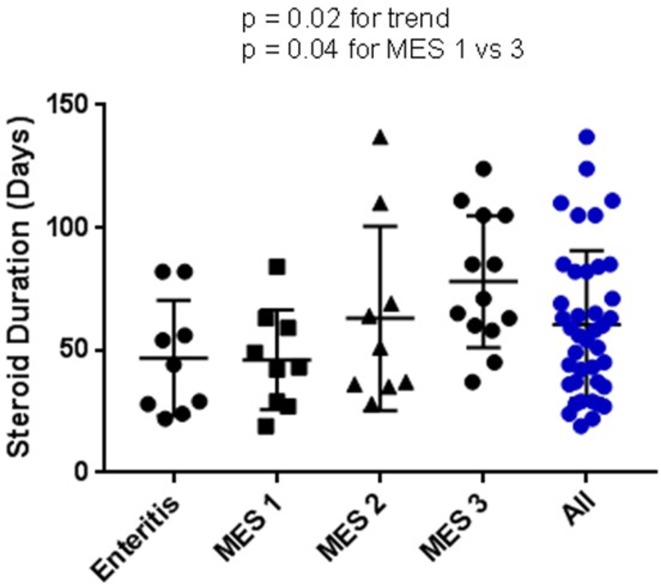
We identified 130 patients with ICI-induced colitis across two institutions. All patients were treated with corticosteroids. Additional and/or alternative immunosuppression was employed in 59 cases, with 52 patients (42%) requiring at least one infusion of infliximab 5 mg/kg. Endoscopic assessment with biopsy was performed in 123 cases of suspected colitis (95%), with 44 cases available for MES tabulation. Presence of ulceration (MES 3) was associated with use of infliximab (p=0.008) and MES was significantly higher in patients who received infliximab compared with those who did not (p=0.003) with a median score of 2.5; conversely, those with an MES of zero rarely required secondary immunosuppression. Notably, symptoms of colitis based on Common Terminology Criteria for Adverse Events grade had no association with endoscopic findings based on MES classification. After adjustment for baseline patient and disease characteristics, there was no significant difference in steroid duration or cancer-related outcomes in patients treated with infliximab.
In our study, we demonstrate the association of endoscopic features, specifically the MES, with immunosuppressive needs. Importantly, we also show that MES was not related to severity of patient symptoms. The data suggest that endoscopic features can guide clinical decision-making better than patient symptoms, both identifying high-risk patients who will require infliximab and those who are likely to respond to initial corticosteroids.
免疫相关性结肠炎是免疫检查点抑制(ICI)的常见且常严重的并发症。尽管对于任何级别的腹泻/结肠炎都不严格推荐进行内镜检查,但新出现的证据表明,内镜评估可能具有重要的治疗意义。在这项回顾性研究中,我们旨在全面描述 ICI 诱导的结肠炎的临床和组织学特征,并特别关注评估内镜的预后作用。
从确诊为 ICI 诱导性结肠炎的 130 名患者的病历中收集数据。在具有内镜和病理数据的患者亚组(n=44)中,使用 Mayo 内镜评分(MES)对内镜数据进行评分,评分范围为 0(无炎症)至 3(结肠溃疡)。使用无进展生存期(PFS)和总生存期(OS)评估英夫利昔单抗对肿瘤治疗效果的影响。
我们在两个机构共发现 130 名 ICI 诱导性结肠炎患者。所有患者均接受皮质类固醇治疗。在 59 例患者中加用了额外的或替代的免疫抑制剂,其中 52 例(42%)至少接受了 1 次英夫利昔单抗 5mg/kg 的输注。对疑似结肠炎的 123 例患者进行了内镜评估和活检,其中 44 例患者可进行 MES 评分。溃疡(MES 3)的存在与英夫利昔单抗的使用相关(p=0.008),与未使用英夫利昔单抗的患者相比,使用英夫利昔单抗的患者 MES 显著更高(p=0.003),中位评分为 2.5;相反,MES 为零的患者很少需要进行二级免疫抑制。值得注意的是,根据不良事件常用术语标准(CTCAE)分级的结肠炎症状与基于 MES 分类的内镜发现无关联。在校正基线患者和疾病特征后,使用英夫利昔单抗的患者在皮质类固醇持续时间或癌症相关结局方面无显著差异。
在我们的研究中,我们证明了内镜特征,特别是 MES,与免疫抑制需求相关。重要的是,我们还表明 MES 与患者症状的严重程度无关。数据表明,内镜特征可以比患者症状更好地指导临床决策,既能识别需要英夫利昔单抗的高危患者,也能识别可能对初始皮质类固醇有反应的患者。