Walter Graham, Kalicinsky Chrystyna, Warrington Richard, Miguel Marianne, Reyes Jeannette, Rubin Tamar S
1Department of Internal Medicine, University of Manitoba, Winnipeg, Canada.
2Section of Allergy and Clinical Immunology, University of Manitoba, Winnipeg, Canada.
Allergy Asthma Clin Immunol. 2020 May 13;16:34. doi: 10.1186/s13223-020-00431-3. eCollection 2020.
Both intravenous and subcutaneous human immune globin G (IgG) replacement (IVIG and SCIG, respectively) reduce severe infection and increase serum IgG levels in primary immune deficiency disorder (PIDD) patients who require replacement. SCIG can be administered either with the aid of an infusion pump, or by patients or caregivers themselves, using butterfly needles and a syringe ("SCIG push"). SCIG offers advantages over IVIG, including higher steady state IgG levels, improved patient quality of life indicators, and decreased cost to the healthcare system, and for these reasons, SCIG has been increasingly used in Manitoba starting in 2007. We sought to determine the effectiveness of SCIG push in our local adult PIDD population.
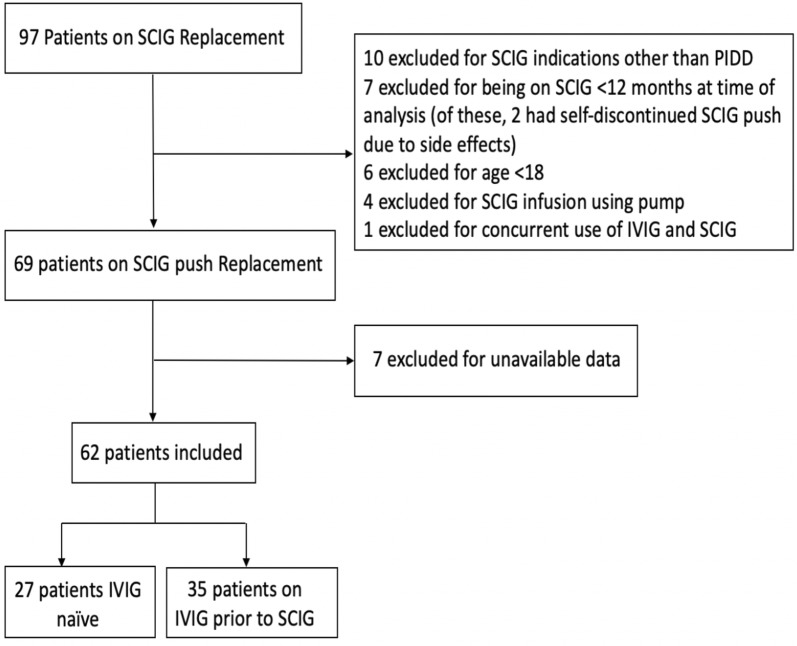
We conducted a retrospective chart review of all adult patients enrolled in the SCIG push program in Manitoba, Canada from its inception in November 2007 through September 2018. We included patients who were naïve to IgG replacement prior to SCIG, and those who had received IVIG immediately prior. We collected data regarding serum IgG levels, antibiotic prescriptions, hospital admissions, and adverse events during a pre-defined period prior to and following SCIG initiation. Statistical significance was determined via two-tailed t-test.
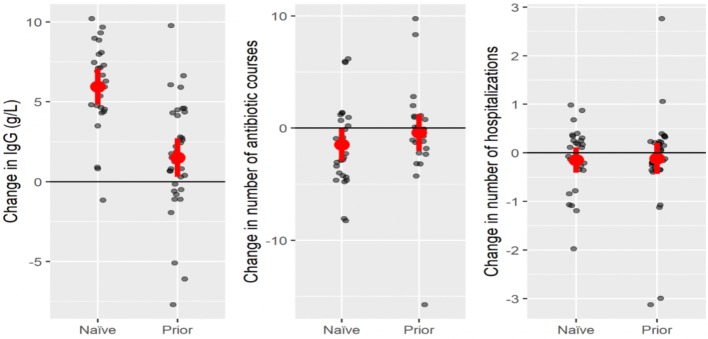
62 patients met inclusion criteria, of whom 35 were on IVIG prior and 27 were IgG replacement naïve. SCIG push resulted in an increase in serum IgG levels in those naïve to IgG replacement, as well as in those who received IVIG prior. SCIG push also resulted in a statistically significant reduction in number of antibiotic prescriptions filled in the naïve subgroup, and no significant change in antibiotics filled in the IVIG prior group. 8/62 PIDD patients (12.9%) left the SCIG program during our review period for varying reasons, including side-effects.
In a real-life setting, in the Manitoba adult PIDD population, SCIG push is an effective method of preventing severe infections, with most patients preferring to continue this therapy once initiated.
静脉注射和皮下注射人免疫球蛋白G(IgG)替代疗法(分别为IVIG和SCIG)可降低严重感染风险,并提高需要替代疗法的原发性免疫缺陷病(PIDD)患者的血清IgG水平。SCIG既可以借助输液泵给药,也可以由患者或护理人员自己使用蝶形针和注射器给药(“SCIG推注”)。SCIG比IVIG具有更多优势,包括更高的稳态IgG水平、改善患者生活质量指标以及降低医疗系统成本,基于这些原因,自2007年起SCIG在曼尼托巴省的使用越来越多。我们试图确定SCIG推注在当地成年PIDD人群中的有效性。
我们对2007年11月该项目启动至2018年9月期间加拿大曼尼托巴省所有参加SCIG推注项目的成年患者进行了回顾性病历审查。我们纳入了在接受SCIG之前未接受过IgG替代治疗的患者,以及之前立即接受过IVIG治疗的患者。我们收集了在SCIG开始之前和之后的预定义时间段内有关血清IgG水平、抗生素处方、住院情况和不良事件的数据。通过双尾t检验确定统计学显著性。
62例患者符合纳入标准,其中35例之前接受过IVIG治疗,27例未接受过IgG替代治疗。SCIG推注使未接受过IgG替代治疗的患者以及之前接受过IVIG治疗的患者的血清IgG水平均有所升高。SCIG推注还使未接受过IgG替代治疗的亚组中开具的抗生素处方数量在统计学上显著减少,而之前接受过IVIG治疗的组中开具的抗生素数量没有显著变化。在我们的审查期间,8/62例PIDD患者(12.9%)因各种原因退出了SCIG项目,包括副作用。
在现实环境中,对于曼尼托巴省的成年PIDD人群,SCIG推注是预防严重感染的有效方法,大多数患者一旦开始治疗就倾向于继续这种疗法。