Division of Cardiology, Cardiothoracovascular Department, Azienda Sanitaria Universitaria Giuliano Isontina, Trieste, Italy.
Institute of Cardiology, University Hospital "S. Orsola-Malpighi", Bologna, Italy.
ESC Heart Fail. 2020 Aug;7(4):1753-1763. doi: 10.1002/ehf2.12737. Epub 2020 May 19.
The optimization of guideline-directed medical therapy (GDMT) in reduced ejection fraction heart failure (HFrEF) is associated with improved survival and can reduce the severity of secondary mitral regurgitation (SMR). Highest tolerated doses should be achieved before percutaneous mitral valve repair (pMVR) and drugs titration further pursued after procedure. The degree of GDMT titration in patients with HFrEF and SMR treated with pMVR remains unexplored. We sought to evaluate the adherence to GDMT in HFrEF in patients undergoing pMVR and to explore the association between changes in GDMT post-pMVR and prognosis.
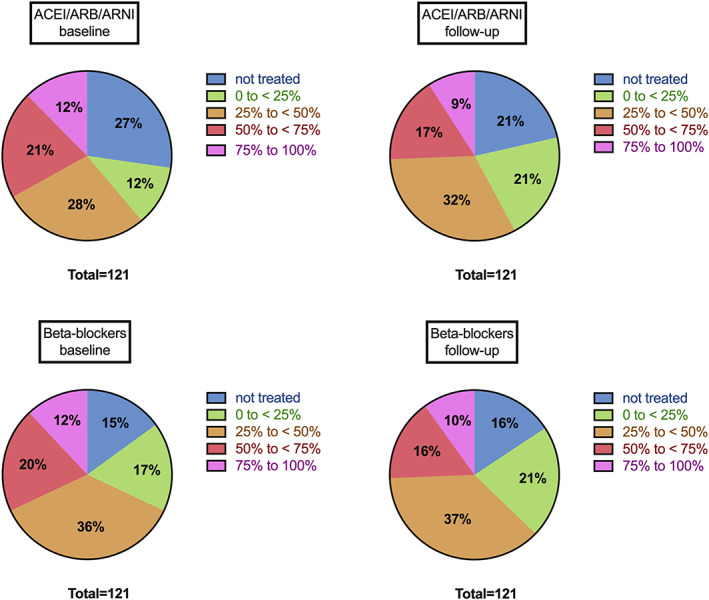
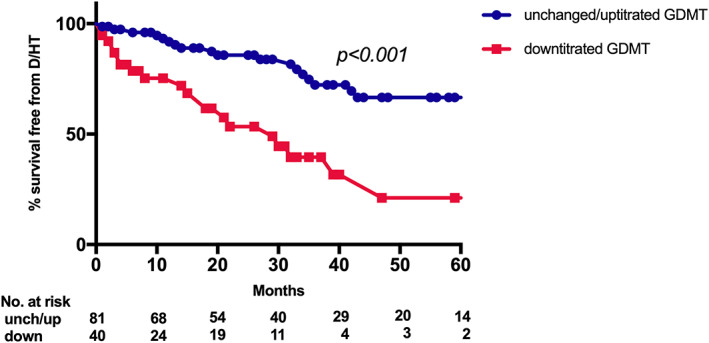
We included all the patients with HFrEF and SMR ≥ 3 + treated with pMVR between 2012 and 2019 and with available follow-up. GDMT, comprehensive of dosages, was systematically recorded. The study endpoint was a composite of death and heart transplantation. Among 133 patients successfully treated, 121 were included (67 ± 12 years old, 77% male patients). Treatment rates of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers/angiotensin receptor neprilysin inhibitor (ACEIs/ARBs/ARNI), beta-blockers, and mineralcorticoid receptor antagonist at baseline and follow-up were 73% and 79%, 85% and 84%, 70% and 70%, respectively. At baseline, 33% and 32% of patients were using >50% of the target dose of ACEI/ARB/ARNI and beta-blockers. At follow-up (median time 4 months), 33% of patients unchanged, 34% uptitrated, and 33% of patients downtitrated GDMT. Downtitration of GDMT was independently associated with higher risk of death/heart transplantation (hazard ratio: 2.542, 95%confidence interval: 1.377-4.694, P = 0.003).
Guideline-directed medical therapy is frequently underdosed in HFrEF patients with SMR undergoing pMVR. Downtitration of medications after procedure is associated with poor prognosis.
射血分数降低的心力衰竭(HFrEF)患者接受指南指导的医学治疗(GDMT)的优化与生存改善相关,并且可以降低继发性二尖瓣反流(SMR)的严重程度。在进行经皮二尖瓣修复术(pMVR)之前,应达到最高耐受剂量,并且在手术后应进一步进行药物滴定。在接受 pMVR 治疗的 HFrEF 合并 SMR 的患者中,GDMT 滴定的程度尚不清楚。我们旨在评估接受 pMVR 治疗的 HFrEF 患者中 GDMT 的依从性,并探讨 pMVR 后 GDMT 变化与预后之间的关系。
我们纳入了 2012 年至 2019 年期间接受 pMVR 治疗且有随访的所有 HFrEF 合并 SMR≥3+的患者。系统记录 GDMT,包括剂量。研究终点为死亡和心脏移植的复合终点。在 133 例成功治疗的患者中,有 121 例纳入(67±12 岁,77%为男性)。在基线和随访时,血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂/血管紧张素受体脑啡肽酶抑制剂(ACEIs/ARBs/ARNI)、β受体阻滞剂和盐皮质激素受体拮抗剂的治疗率分别为 73%和 79%、85%和 84%、70%和 70%。基线时,33%和 32%的患者使用 ACEI/ARB/ARNI 和β受体阻滞剂的目标剂量>50%。在随访(中位数时间 4 个月)时,33%的患者 GDMT 未改变,34%的患者剂量增加,33%的患者剂量减少。GDMT 的剂量减少与死亡/心脏移植的风险增加独立相关(危险比:2.542,95%置信区间:1.377-4.694,P=0.003)。
在接受 pMVR 的 HFrEF 合并 SMR 患者中,GDMT 经常剂量不足。手术后药物剂量减少与预后不良相关。