Service de Pneumologie, Institut du Thorax, CHU de Nantes, Nantes, France.
Service de Pneumologie, CHU Dupuytren, Limoges, France.
Int J Chron Obstruct Pulmon Dis. 2020 Apr 30;15:949-962. doi: 10.2147/COPD.S236787. eCollection 2020.
To characterise patients with chronic obstructive pulmonary disease (COPD) who are rehospitalised for an acute exacerbation, to estimate the cost of these hospitalisations, to characterise high risk patient sub groups and to identify factors potentially associated with the risk of rehospitalisation.
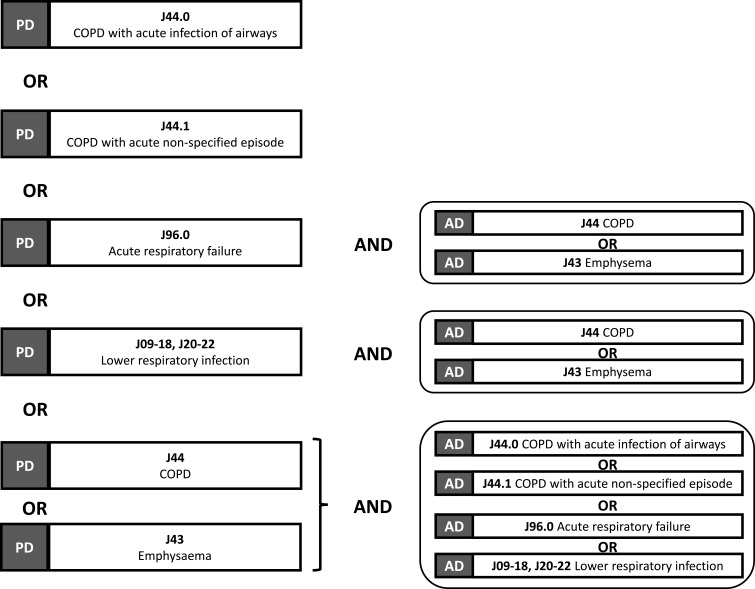
This was a retrospective study using the French National Hospital Discharge Database. All patients aged ≥40 years hospitalised for an acute exacerbation of COPD between 2015 and 2016 were identified and followed for six months. Patients with at least one rehospitalisation for acute exacerbation of COPD constituted the rehospitalisation analysis population. A machine learning model was built to study the factors associated with the risk of rehospitalisation using decision tree analysis. A direct cost analysis was performed from the perspective of national health insurance.
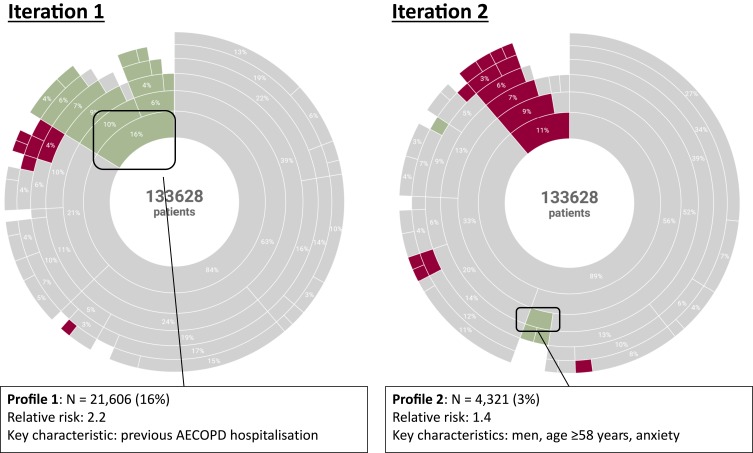
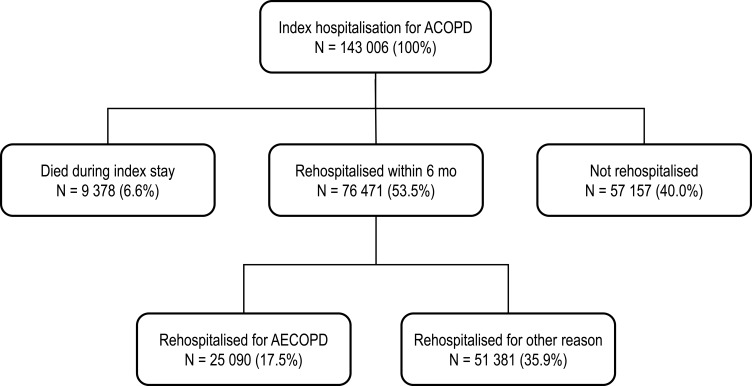
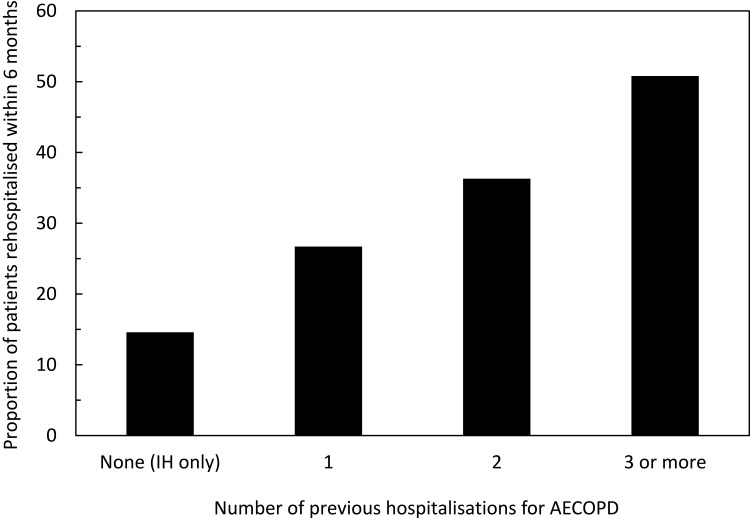
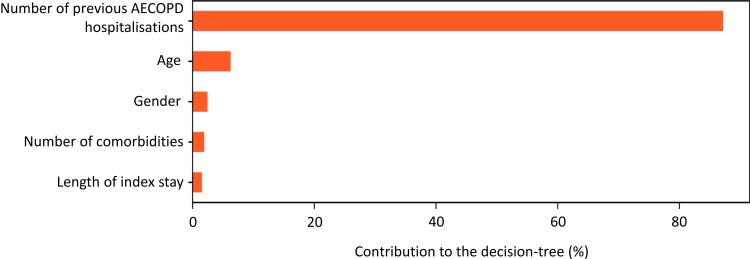
A total of 143,006 eligible patients were hospitalised for an acute exacerbation of COPD (AECOPD) in 2015-2016 (mean age: 74 years; 62.1% men). 25,090 (18.8%) were rehospitalised for another exacerbation within six months. In this study, 8.5% of patients died during or immediately following the index hospitalisation and 10.5% died during or immediately after rehospitalisation ( <0.001). The specific cost of these rehospitalisations was € 5304. The overall total cost per patient of all AECOPD-related stays was € 9623, being significantly higher in patients who were rehospitalised (€ 16,275) compared to those who were not (€ 8208). In decision tree analysis, the most important driver of rehospitalisation was hospitalisation in the previous two years (contributing 85% of the information).
Rehospitalisations for acute exacerbations of COPD carry a high epidemiological and economic burden. Since hospitalisation for an acute exacerbation is the most important determinant of future rehospitalisations, management of COPD needs to focus on interventions aimed at decreasing the rehospitalisation risk of in order to lower the burden of disease.
描述因慢性阻塞性肺疾病(COPD)急性加重而再次住院的患者,估算这些住院的费用,描述高危患者亚组的特征,并确定与再住院风险相关的潜在因素。
这是一项使用法国国家住院数据库的回顾性研究。在 2015 年至 2016 年期间,我们确定了所有因 COPD 急性加重而住院的年龄≥40 岁的患者,并对他们进行了 6 个月的随访。至少有一次因 COPD 急性加重再次住院的患者构成了再住院分析人群。使用决策树分析构建了一个机器学习模型,以研究与再住院风险相关的因素。从国家健康保险的角度进行了直接成本分析。
2015-2016 年,共有 143006 名符合条件的患者因 COPD 急性加重(AECOPD)住院(平均年龄:74 岁;62.1%为男性)。25090 名(18.8%)在 6 个月内因另一次加重而再次住院。在这项研究中,8.5%的患者在指数住院期间或之后立即死亡,10.5%的患者在再次住院期间或之后立即死亡(<0.001)。这些再住院的特定费用为 5304 欧元。所有与 AECOPD 相关住院的每位患者的总费用为 9623 欧元,再住院患者(16275 欧元)显著高于未再住院患者(8208 欧元)。在决策树分析中,再住院的最重要驱动因素是前两年的住院(占信息的 85%)。
COPD 急性加重的再住院治疗负担沉重。由于急性加重住院是未来再住院的最重要决定因素,因此 COPD 的管理需要重点关注降低再住院风险的干预措施,以降低疾病负担。