Lopez-Siles Mireia, Aldeguer Xavier, Sabat-Mir Miriam, Serra-Pagès Mariona, Duncan Sylvia H, Flint Harry J, Garcia-Gil L Jesús, Martinez-Medina Margarita
Laboratory of Molecular Microbiology, Biology Department, Universitat de Girona, Girona 17003, Spain.
Department of Gastroenterology, Hospital Universitari Dr. Josep Trueta, Girona 17007, Spain.
World J Gastrointest Pathophysiol. 2020 May 12;11(3):64-77. doi: 10.4291/wjgp.v11.i3.64.
The challenges for inflammatory bowel disease (IBD) diagnostics are to discriminate it from gut conditions with similar symptoms such as irritable bowel syndrome (IBS), to distinguish IBD subtypes, to predict disease progression, and to establish the risk to develop colorectal cancer (CRC). Alterations in gut microbiota have been proposed as a source of information to assist in IBD diagnostics. (), its phylogroups, and () have been reported as potential biomarkers, but their performance in challenging IBD diagnostic situations remains elusive. We hypothesize that bacterial biomarkers based in these species may help to discriminate these conditions of complex diagnostics.
To evaluate the usefulness of indices calculated from the quantification of these species as biomarkers to aid in IBD diagnostics.
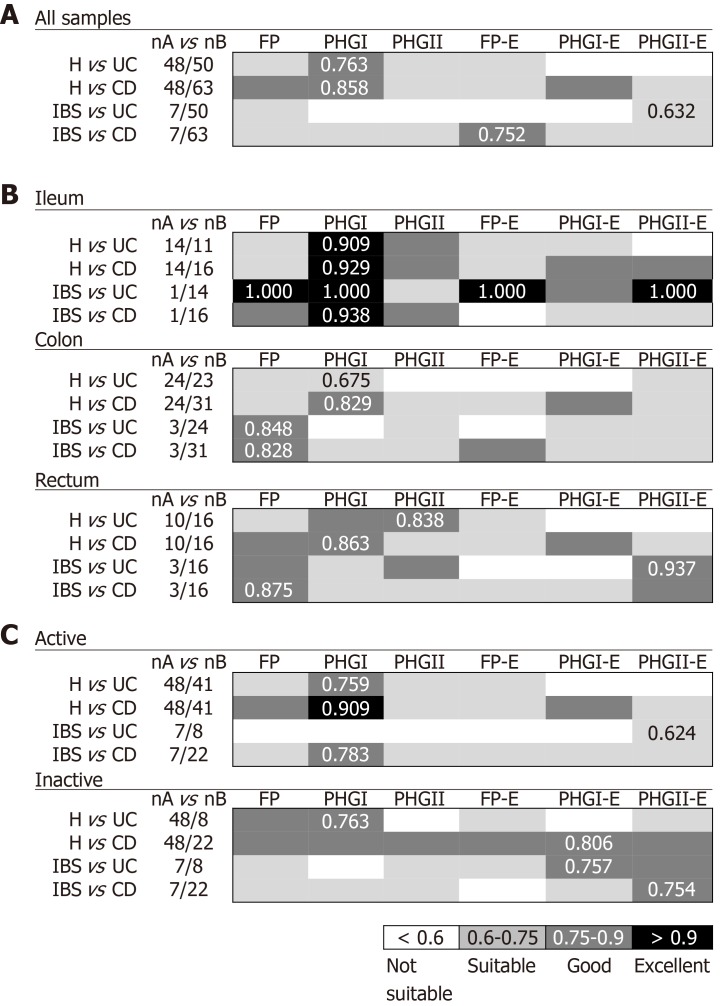
A retrospective study of 131 subjects (31 controls (H); 45 Crohn's disease (CD), 25 ulcerative colitis (UC), 10 IBS, and 20 CRC patients) was performed to assess the usefulness of bacterial biomarkers in biopsies. Further, the performance of biomarkers in faeces was studied in 29 stool samples (19 CD, 10 UC). Relative abundances of total (FP), its phylogroups (PHGI and PHGII), and (E) quantification were determined by qPCR. Loads were combined to calculate the FP-E index, the PHGI-E index and the PHGII-E index. Biomarkers accuracy to discriminate among conditions was measured by the area under the receiver operating characteristic curve (AUC).
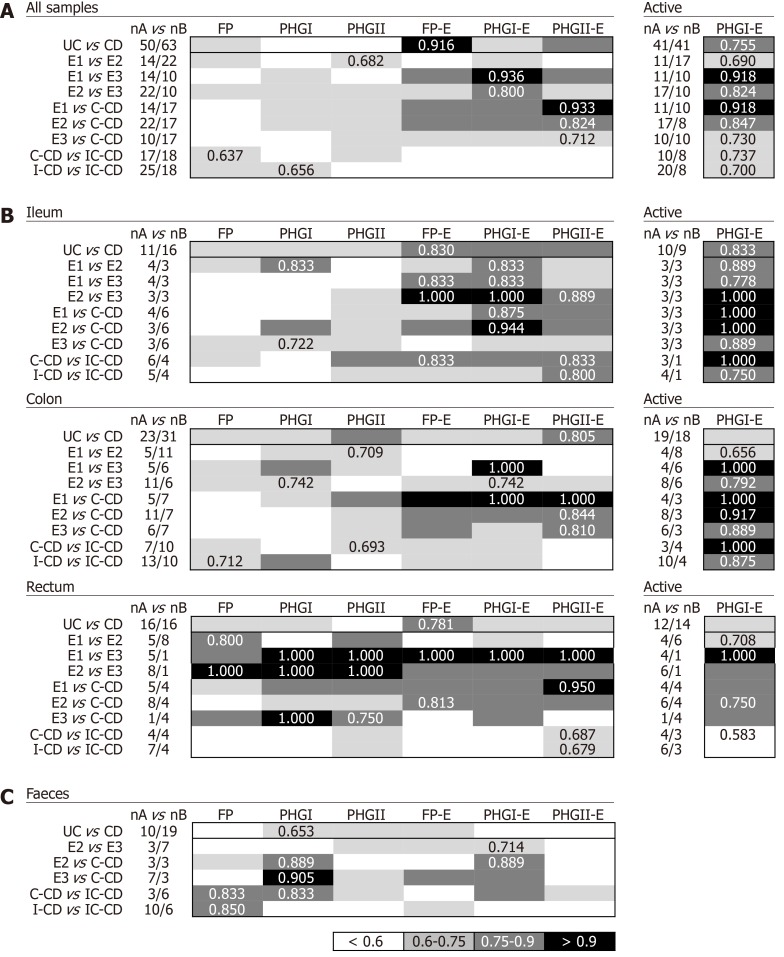
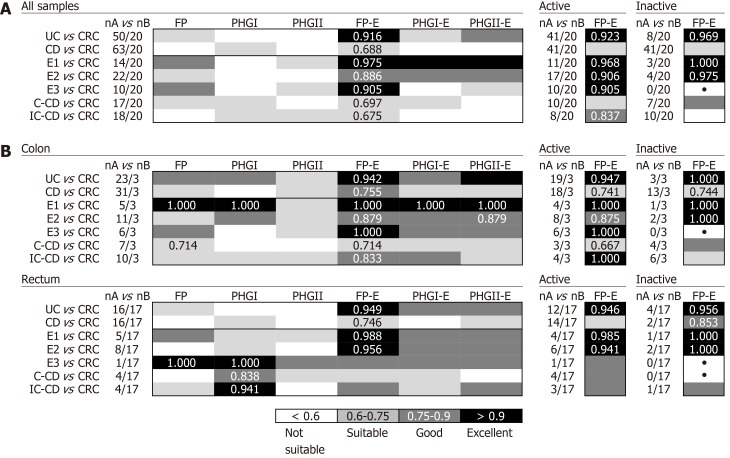
In biopsies, FP-E index was good for discriminating IBS from CD (AUC = 0.752) while PHGII-E index was suitable for discriminating IBS from UC (AUC = 0.632). The FP-E index would be the choice to discriminate IBD from CRC, especially from all UC subtypes (AUC ≥ 0.875), regardless of the activity status of the patient. Discrimination between UC patients that had the longest disease duration and those with CRC featured slightly lower AUC values. Concerning differentiation in IBD with shared location, PHGI-E index can establish progression from proctitis and left-sided colitis to ulcerative pancolitis (AUC ≥ 0.800). PHG I-E index analysis in tissue would be the choice to discriminate within IBD subtypes of shared location (AUC ≥ 0.712), while in non-invasive faecal samples FP or PHGI could be good indicators (AUC ≥ 0.833).
phylogroups combined with offer potential to discriminate between IBD and CRC patients and can assist in IBD subtypes classification, which may help in solving IBD diagnostics challenges.
炎症性肠病(IBD)诊断面临的挑战包括将其与具有相似症状的肠道疾病(如肠易激综合征(IBS))相区分,辨别IBD亚型,预测疾病进展,以及确定患结直肠癌(CRC)的风险。肠道微生物群的改变已被认为是有助于IBD诊断的信息来源。()、其菌群分类以及()已被报道为潜在的生物标志物,但其在具有挑战性的IBD诊断情况下的表现仍不明确。我们假设基于这些物种的细菌生物标志物可能有助于区分这些复杂诊断的情况。
评估从这些物种的定量计算得出的指标作为生物标志物在辅助IBD诊断方面的有用性。
对131名受试者(31名对照(H);45名克罗恩病(CD)患者、25名溃疡性结肠炎(UC)患者、10名IBS患者和20名CRC患者)进行回顾性研究,以评估活检中细菌生物标志物的有用性。此外,在29份粪便样本(19份CD样本、10份UC样本)中研究了生物标志物在粪便中的表现。通过定量聚合酶链反应(qPCR)确定总(FP)、其菌群分类(PHGI和PHGII)以及(E)定量的相对丰度。将这些负荷量结合起来计算FP - E指数、PHGI - E指数和PHGII - E指数。通过受试者操作特征曲线(AUC)下的面积来衡量生物标志物在不同情况之间进行区分的准确性。
在活检中,FP - E指数有助于区分IBS和CD(AUC = 0.752),而PHGII - E指数适用于区分IBS和UC(AUC = 0.632)。FP - E指数将是区分IBD和CRC,特别是区分所有UC亚型(AUC≥0.875)的选择,无论患者的活动状态如何。病程最长的UC患者与CRC患者之间的区分,AUC值略低。关于在相同发病部位的IBD中的区分,PHGI - E指数可以确定从直肠炎和左侧结肠炎到全结肠炎的进展(AUC≥0.800)。在组织中进行PHG I - E指数分析将是区分相同发病部位的IBD亚型(AUC≥0.712)的选择,而在非侵入性粪便样本中,FP或PHGI可能是良好的指标(AUC≥0.833)。
菌群分类与相结合有潜力区分IBD和CRC患者,并有助于IBD亚型分类,这可能有助于解决IBD诊断难题。