Department of Anesthesiology and Pain Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro Gangnam-gu, Seoul, 06351, South Korea.
Sci Rep. 2020 May 21;10(1):8449. doi: 10.1038/s41598-020-65532-w.
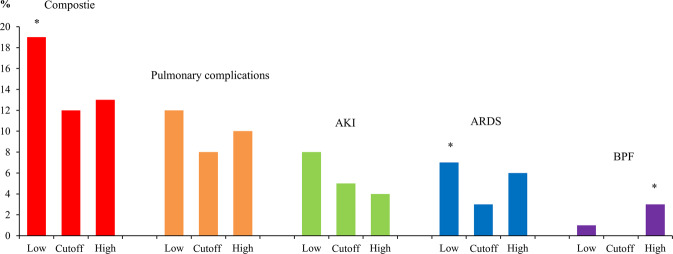
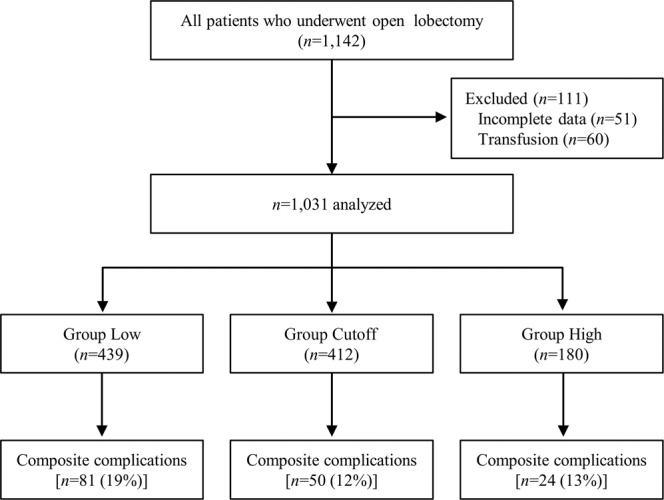
Restrictive fluid management has been recommended for thoracic surgery. However, specific guidelines are lacking, and there is always concern regarding impairment of renal perfusion with a restrictive policy. The objective of this study was to find the net intraoperative fluid infusion rate which shows the lowest incidence of composite complications (either pulmonary complications or acute kidney injury) in open thoracotomy. We hypothesized that a certain range of infusion rate would decrease the composite complications within postoperative 30 days. All patients (n = 1,031) who underwent open thoracotomy at a tertiary care university hospital were included in this retrospective study. The time frame of fluid monitoring was from the start of operation to postoperative 24 hours. The cutoff value of the intraoperative net fluid amount was 4-5 ml.kg.h according to the minimum p-value method, thus, patients were divided into Low (≤3 ml.kg.h), Cutoff (4-5 ml.kg.h) and High (≥6 ml.kg.h) groups. The Cutoff group showed the lowest composite complication rate (19%, 12%, and 13% in the Low, Cutoff, and High groups, respectively, P = 0.0283; Low vs. Cutoff, P = 0.0324, Bonferroni correction). Acute respiratory distress syndrome occurred least frequently in the Cutoff group (7%, 3%, and 6% for the Low, Cutoff, and High groups, respectively, P = 0.0467; Low vs. Cutoff, P = 0.0432, Bonferroni correction). In multivariable analysis, intraoperative net fluid infusion rate was associated with composite complications, and the Cutoff group decreased risk (odds ratio 0.54, 95% confidence interval: 0.35-0.81, P = 0.0035). In conclusion, maintaining intraoperative net fluid infusion at 4-5 ml.kg.h was associated with better results in open thoracotomy, in terms of composite complications, compared to more restrictive fluid management.
限制液体管理已被推荐用于胸外科手术。然而,目前缺乏具体的指南,而且人们一直担心限制液体管理策略会损害肾脏灌注。本研究的目的是确定开胸手术中净术中液体输注率最低的复合并发症(肺部并发症或急性肾损伤)。我们假设一定范围的输液率将降低术后 30 天内的复合并发症。所有在三级护理大学医院接受开胸手术的患者(n=1031)均纳入本回顾性研究。液体监测的时间范围为手术开始至术后 24 小时。根据最小 p 值法,术中净液体量的截止值为 4-5ml/kg/h,因此患者分为低(≤3ml/kg/h)、截止(4-5ml/kg/h)和高(≥6ml/kg/h)组。截止组的复合并发症发生率最低(低、截止和高组分别为 19%、12%和 13%,P=0.0283;低与截止,P=0.0324,Bonferroni 校正)。急性呼吸窘迫综合征在截止组中发生率最低(低、截止和高组分别为 7%、3%和 6%,P=0.0467;低与截止,P=0.0432,Bonferroni 校正)。多变量分析显示,术中净液体输注率与复合并发症相关,截止组降低了风险(比值比 0.54,95%置信区间:0.35-0.81,P=0.0035)。总之,与更严格的液体管理相比,在开胸手术中维持 4-5ml/kg/h 的术中净液体输注与复合并发症的更好结果相关。