Centre for Pulmonary Hypertension at Thoraxklinik gGmbH at Heidelberg University Hospital, Röntgenstraße 1, 69126, Heidelberg, Germany.
Translational Lung Research Centre Heidelberg (TLRC), German Centre for Lung Research (DZL), Heidelberg, Germany.
Respir Res. 2020 May 24;21(1):127. doi: 10.1186/s12931-020-01393-1.
The objective of this study was to analyze prognostic factors and risk stratification in patients with pulmonary arterial hypertension (PAH) and comorbidities.
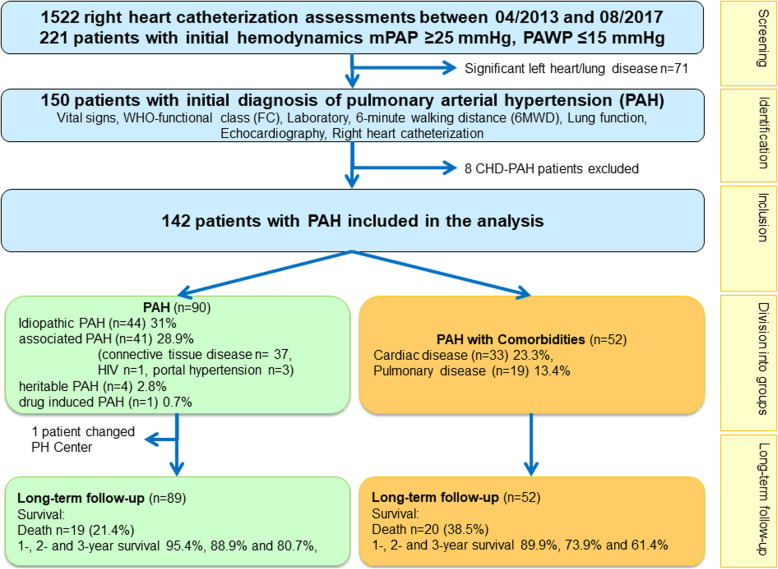
Patients with invasively diagnosed PAH were included in the analysis. Comorbidities were clinically diagnosed as proposed in the 6th World Symposium of pulmonary hypertension. Uni- and multivariate analysis were employed for identification of factors predicting survival and time to first clinical worsening (TTCW). Risk stratification was based on parameters from ESC/ERS-guidelines 2015.
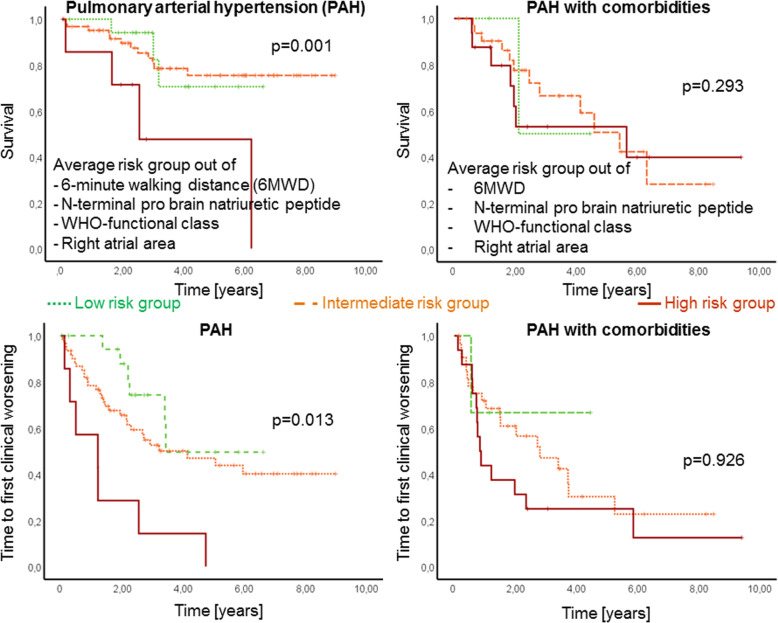
In total 142 patients were enrolled in the study, 90 of them were diagnosed as PAH without and 52 with comorbidities. All patients received targeted PAH therapy and were followed for 3.3 ± 2.4 years. In PAH patients without comorbidities survival and TTCW were significantly associated with reduced 6-min walking distance (6MWD), elevated N-terminal pro brain natriuretic peptide (NT-proBNP), WHO-functional class (WHO-FC) and right atrial (RA) area. In the multivariate analysis, 6MWD was an independent predictor for survival (p = 0.002) and WHO-FC for TTCW (p = 0.001). In patients with PAH and comorbidities these parameters had no significant association with survival and TTCW. Average risk score was significantly associated with survival (p = 0.001) and TTCW (p = 0.013) in PAH but not in PAH with comorbidities (both p > 0.05; figure 1).
Risk stratification based on ESC/ERS-guidelines could only be confirmed in patients without comorbidities, but not in patients with PAH and comorbidities. The data of this study suggest, that a different risk stratification needs to be applied to PAH patients with comorbidities. Further studies are needed to confirm these results.
Not applicable, retrospective registry.
本研究旨在分析合并症的肺动脉高压(PAH)患者的预后因素和风险分层。
本研究纳入了经有创诊断的 PAH 患者。合并症按照第 6 届世界肺动脉高压研讨会提出的标准进行临床诊断。采用单因素和多因素分析来确定预测生存和首次临床恶化时间(TTCW)的因素。风险分层基于 2015 年 ESC/ERS 指南中的参数。
本研究共纳入 142 例患者,其中 90 例诊断为无合并症的 PAH,52 例诊断为合并症的 PAH。所有患者均接受了靶向 PAH 治疗,并随访了 3.3±2.4 年。在无合并症的 PAH 患者中,生存和 TTCW 与 6 分钟步行距离(6MWD)减少、N 末端脑利钠肽前体(NT-proBNP)升高、WHO 功能分级(WHO-FC)和右心房(RA)面积增加显著相关。在多因素分析中,6MWD 是生存的独立预测因素(p=0.002),而 WHO-FC 是 TTCW 的独立预测因素(p=0.001)。在合并症的 PAH 患者中,这些参数与生存和 TTCW 无显著相关性。平均风险评分与 PAH 患者的生存(p=0.001)和 TTCW(p=0.013)显著相关,但与合并症的 PAH 患者无关(均 p>0.05;图 1)。
基于 ESC/ERS 指南的风险分层仅在无合并症的患者中得到确认,而在合并症的 PAH 患者中则无法得到确认。本研究的数据表明,需要对合并症的 PAH 患者应用不同的风险分层。需要进一步的研究来证实这些结果。
不适用,回顾性注册。