McGovern Andrew P, Hogg Michael, Shields Beverley M, Sattar Naveed A, Holman Rury R, Pearson Ewan R, Hattersley Andrew T, Jones Angus G, Dennis John M
University of Exeter Medical School, Institute of Biomedical and Clinical Science, University of Exeter, Exeter, Devon, UK
University of Exeter Medical School, Institute of Biomedical and Clinical Science, University of Exeter, Exeter, Devon, UK.
BMJ Open Diabetes Res Care. 2020 May;8(1). doi: 10.1136/bmjdrc-2020-001238.
To identify risk factors, absolute risk, and impact on treatment discontinuation of genital infections with sodium-glucose co-transporter-2 inhibitors (SGLT2i).
We assessed the relationship between baseline characteristics and genital infection in 21 004 people with type 2 diabetes initiating SGLT2i and 55 471 controls initiating dipeptidyl peptidase-4 inhibitors (DPP4i) in a UK primary care database. We assessed absolute risk of infection in those with key risk factors and the association between early genital infection and treatment discontinuation.
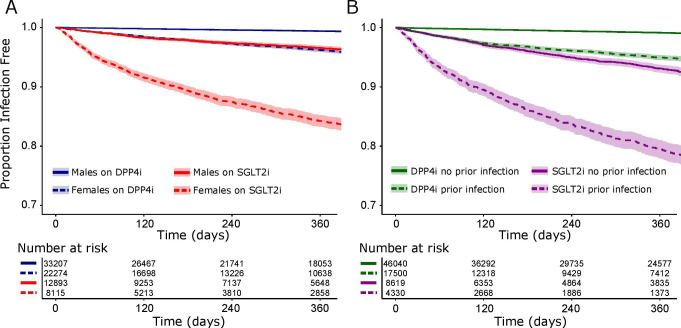
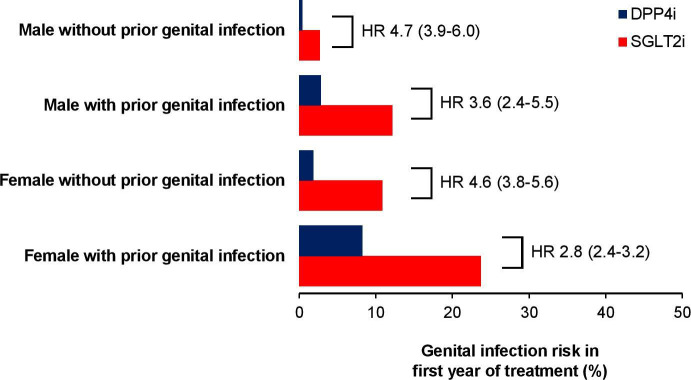
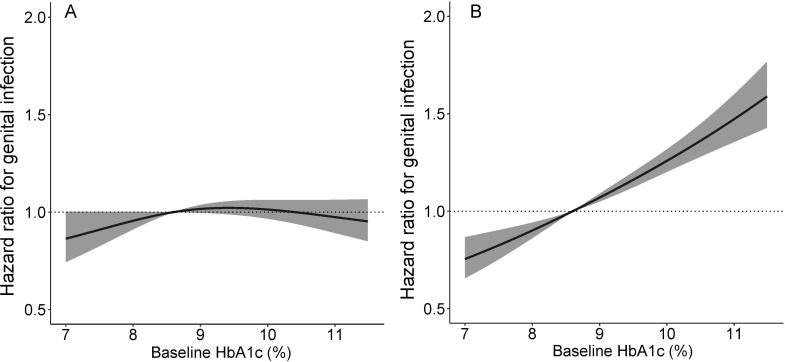
Genital infection was substantially more common in those treated with SGLT2i (8.1% within 1 year) than DPP4i (1.8%). Key predictors of infection with SGLT2i were female sex (HR 3.64; 95% CI 3.23 to 4.11) and history of genital infection; <1 year before initiation (HR 4.38; 3.73 to 5.13), 1-5 years (HR 3.04; 2.64 to 3.51), and >5 years (HR 1.79; 1.55 to 2.07). Baseline HbA was not associated with infection risk for SGLT2i, in contrast to DPP4i where risk increased with higher HbA. One-year absolute risk of genital infection with SGLT2i was highest for those with a history of prior infection (females 23.7%, males 12.1%), compared with those without (females 10.8%, males 2.7%). Early genital infection was associated with a similar discontinuation risk for SGLT2i (HR 1.48; 1.21-1.80) and DPP4i (HR 1.58; 1.21-2.07).
Female sex and history of prior infection are simple features that can identify subgroups at greatly increased risk of genital infections with SGLT2i therapy. These data can be used to risk-stratify patients. High HbA is not a risk factor for genital infections with SGLT2i.
确定钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)治疗生殖器感染的危险因素、绝对风险以及对治疗中断的影响。
在英国初级医疗数据库中,我们评估了21004例开始使用SGLT2i的2型糖尿病患者和55471例开始使用二肽基肽酶4抑制剂(DPP4i)的对照者的基线特征与生殖器感染之间的关系。我们评估了具有关键危险因素者的感染绝对风险以及早期生殖器感染与治疗中断之间的关联。
使用SGLT2i治疗的患者中生殖器感染(1年内发生率8.1%)比使用DPP4i治疗的患者(1.8%)更为常见。SGLT2i治疗感染的关键预测因素为女性(HR 3.64;95%CI 3.23至4.11)和生殖器感染史;开始治疗前<1年(HR 4.38;3.73至5.13)、1 - 5年(HR 3.04;2.64至3.51)以及>5年(HR 1.79;1.55至2.07)。与DPP4i不同,DPP4i的感染风险随糖化血红蛋白(HbA)升高而增加,而SGLT2i治疗的基线HbA与感染风险无关。与无生殖器感染史者相比(女性10.8%,男性2.7%),有生殖器感染史者使用SGLT2i治疗1年的生殖器感染绝对风险最高(女性23.7%,男性12.1%)。早期生殖器感染与SGLT2i(HR 1.48;1.21 - 1.80)和DPP4i(HR 1.58;1.21 - 2.07)的治疗中断风险相似。
女性和既往感染史是可识别SGLT2i治疗生殖器感染风险大幅增加亚组的简单特征。这些数据可用于对患者进行风险分层。高HbA不是SGLT2i治疗生殖器感染的危险因素。