Laboratory and Clinical Research Institute for Pain, Department of Anaesthesiology, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Queen Mary Hospital, Room 424, Block K, 102, Pokfulam Road, Hong Kong SAR, China.
Department of Orthopaedics and Traumatology, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China.
BMC Anesthesiol. 2020 May 28;20(1):130. doi: 10.1186/s12871-020-01044-4.
It is unclear whether regional anesthesia with infraclavicular nerve block or general anesthesia provides better postoperative analgesia after distal radial fracture fixation, especially when combined with regular postoperative analgesic medications. The aim of this study was to compare the postoperative analgesic effects of regional versus general anesthesia.
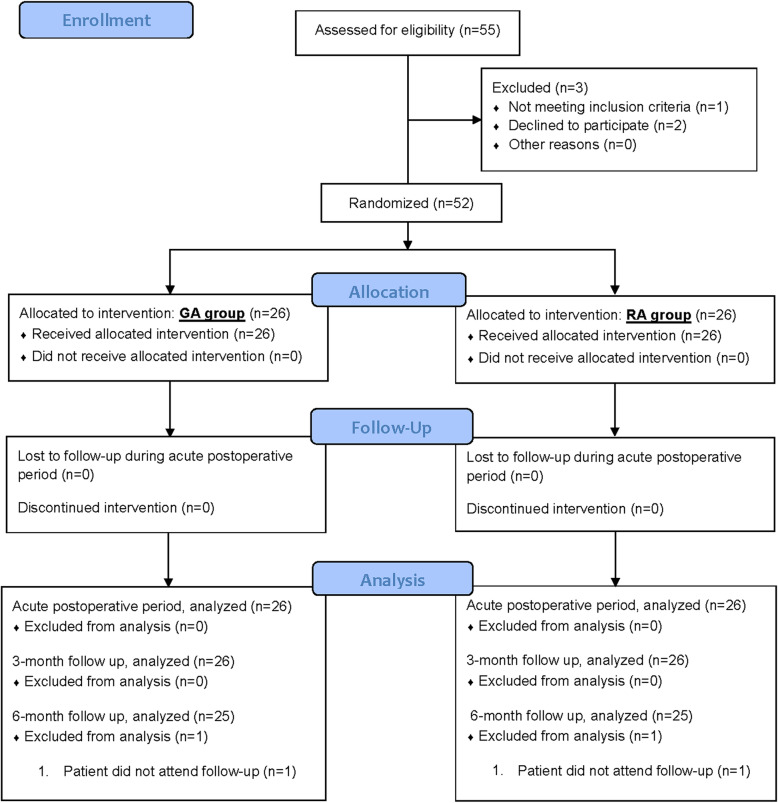
In this prospective, observer blinded, randomized controlled trial, 52 patients undergoing distal radial fracture fixation received either general anesthesia (n = 26) or regional anesthesia (infraclavicular nerve block, n = 26). Numerical rating scale pain scores, analgesic consumption, patient satisfaction, adverse effects, upper limb functional scores (Patient-Rated Wrist Evaluation, QuickDASH), health related quality of life (SF12v2), and psychological status were evaluated after surgery.
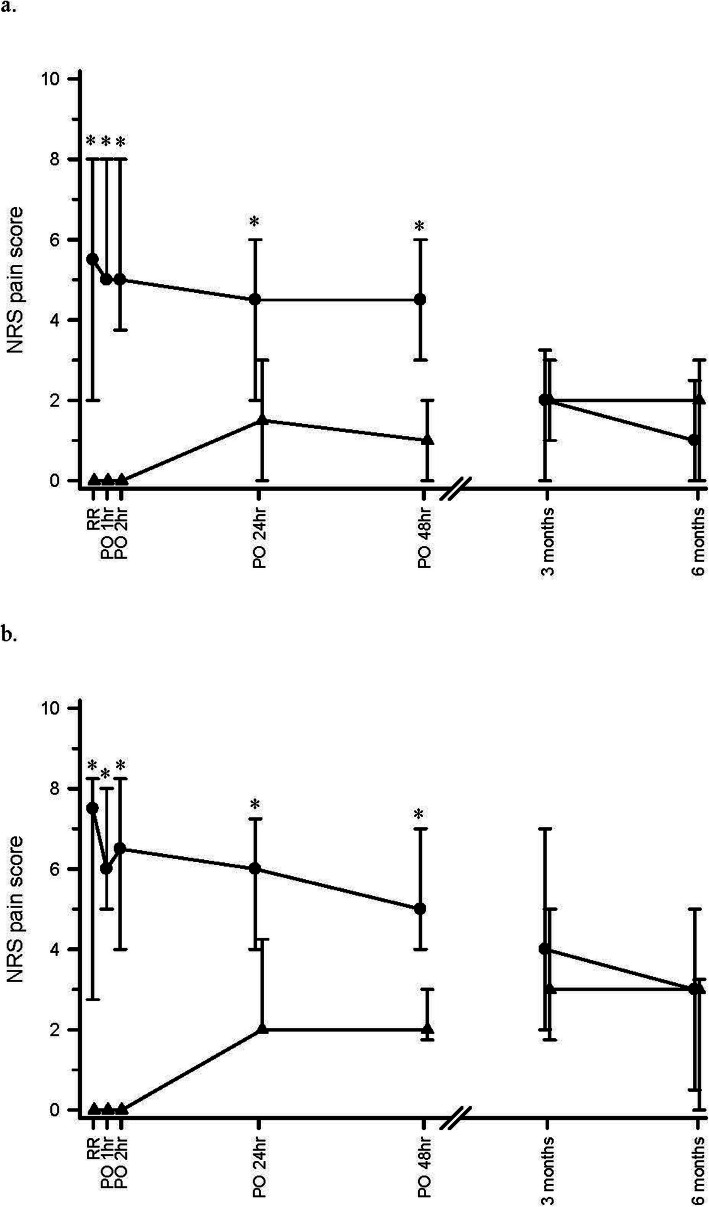
Regional anesthesia was associated with significantly lower pain scores both at rest and with movement on arrival to the post-anesthetic care unit; and at 1, 2, 24 and 48 h after surgery (p ≤ 0.001 at rest and with movement). Morphine consumption in the post-anesthetic care unit was significantly lower in the regional anesthesia group (p<0.001). There were no differences in oral analgesic consumption. Regional anesthesia was associated with lower incidences of nausea (p = 0.004), and vomiting (p = 0.050). Patient satisfaction was higher in the regional anesthesia group (p = 0.003). There were no long-term differences in pain scores and other patient outcomes.
Regional anesthesia with ultrasound guided infraclavicular nerve block was associated with better acute pain relief after distal radial fracture fixation, and may be preferred over general anesthesia.
Before subject enrollment, the study was registered at ClinicalTrials.gov (NCT03048214) on 9th February 2017.
在联合常规术后镇痛药物使用的情况下,对于桡骨远端骨折固定术后,局部麻醉下锁骨下神经阻滞与全身麻醉相比,哪种方式能提供更好的术后镇痛效果尚不清楚。本研究旨在比较区域麻醉与全身麻醉的术后镇痛效果。
这是一项前瞻性、观察者设盲、随机对照试验,共纳入 52 例行桡骨远端骨折固定术的患者,分为全身麻醉组(n=26)和区域麻醉组(锁骨下神经阻滞,n=26)。术后评估两组患者的数字评分量表(NRS)疼痛评分、镇痛药物消耗、患者满意度、不良反应、上肢功能评分(腕关节患者报告评分、简易上肢功能测试)、健康相关生活质量(SF-12v2)和心理状态。
与全身麻醉相比,区域麻醉在到达麻醉后恢复室时、静息状态和活动时,以及术后 1、2、24 和 48 小时的疼痛评分显著更低(静息和活动时,p≤0.001)。区域麻醉组在麻醉后恢复室的吗啡消耗量显著降低(p<0.001)。两组患者口服镇痛药的消耗量无差异。区域麻醉组恶心(p=0.004)和呕吐(p=0.050)的发生率更低。区域麻醉组患者满意度更高(p=0.003)。两组患者在疼痛评分和其他患者结局方面无长期差异。
超声引导锁骨下神经阻滞的区域麻醉可更好地缓解桡骨远端骨折固定术后的急性疼痛,可能优于全身麻醉。
在患者入组前,该研究于 2017 年 2 月 9 日在 ClinicalTrials.gov 上注册(NCT03048214)。