Chao Bei, Ju Xiaoli, Zhang Lirong, Xu Xin, Zhao Yan
Department of Clinical Laboratory, The Third Affiliated Hospital of Soochow University, Changzhou, China.
Histoembryology, Jiangsu University, Zhenjiang, China.
Front Oncol. 2020 May 13;10:766. doi: 10.3389/fonc.2020.00766. eCollection 2020.
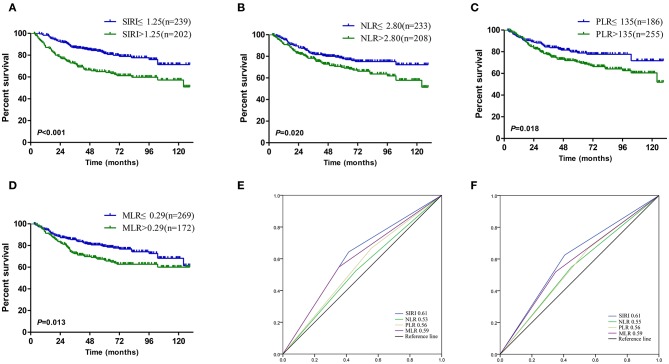
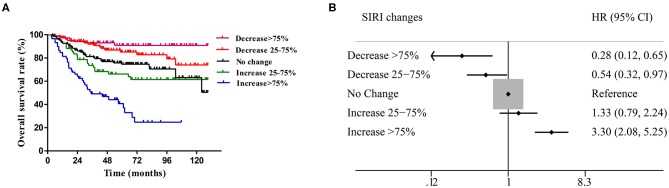
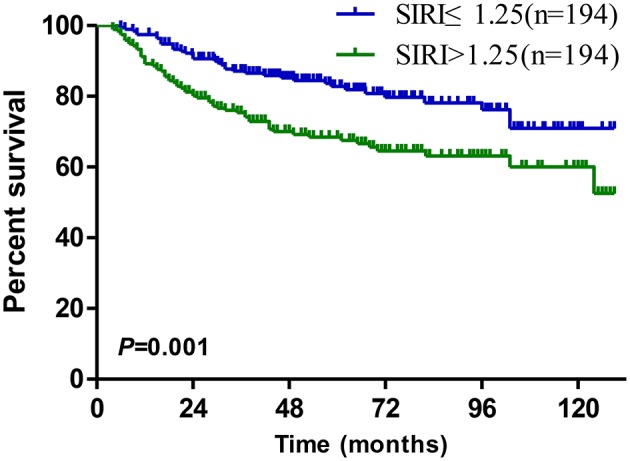
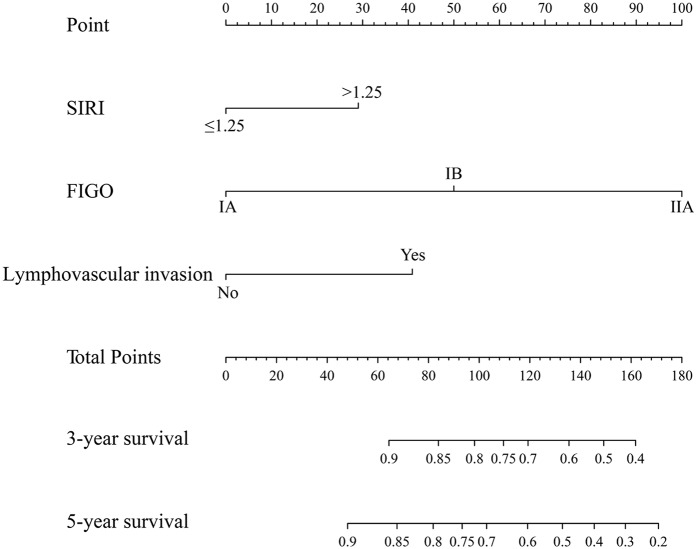
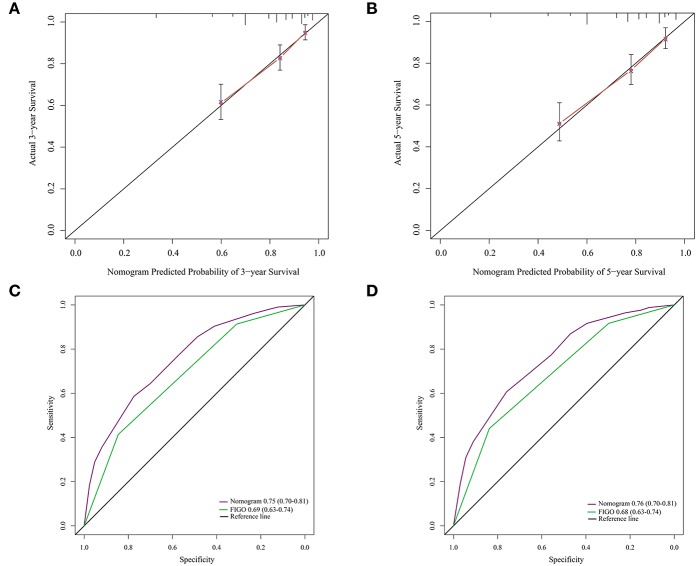
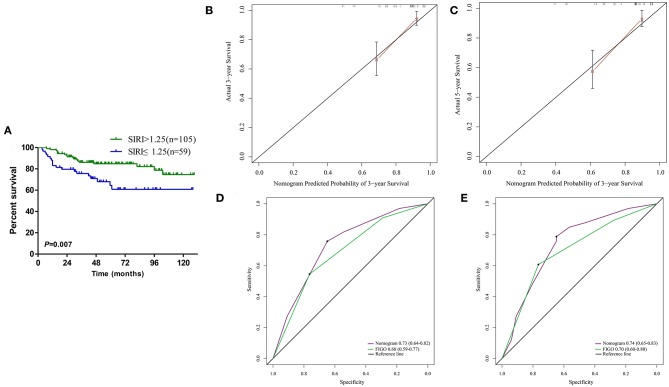
It has been confirmed that the systemic inflammation response index (SIRI) based on peripheral blood neutrophil, monocyte and lymphocyte counts can be used for the prognostication of patients with various malignant tumors. However, the prognostic value of SIRI in cervical cancer patients has not yet been reported. This study found that a higher SIRI was related to lymphovascular invasion and was also significantly associated with FIGO stage, radiotherapy, neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), and monocyte/lymphocyte ratio (MLR) but not related to other clinical and pathological parameters. According to the Kaplan-Meier survival analysis, a high SIRI was associated with the poor prognosis of cervical cancer patients in the primary and validation groups. SIRI, NLR, PLR, and MLR can all be used to determine the prognosis of patients with operable cervical cancer. Moreover, it was confirmed that only SIRI was an independent prognostic factor for patients with operable cervical cancer. The same result was obtained in the propensity score matching (PSM) analysis. In the ROC curve analysis, SIRI was more accurate in predicting the prognosis of cervical cancer patients. Then, a nomogram was established based on SIRI, FIGO stage and lymphovascular invasion, which could determine the prognosis of cervical cancer patients more accurately than FIGO stage. The validation cohort showed the same results. In addition, the changes in SIRI relative to the baseline value at 4-8 weeks after surgery were closely related to the survival of cervical cancer patients. Compared with those with unchanged SIRI (absolute value of variation <25%), cervical cancer patients with an increase in SIRI > 75% had worse OS ( < 0.001), while patients with a decrease in SIRI > 75% had a better prognosis ( < 0.001). SIRI can serve as a new independent prognostic index and a potential marker for therapeutic response monitoring in patients with curable cervical cancer. Compared with the traditional FIGO staging system, the nomogram integrating SIRI can predict the survival of cervical cancer patients more objectively and reliably after radical surgery.
已经证实,基于外周血中性粒细胞、单核细胞和淋巴细胞计数的全身炎症反应指数(SIRI)可用于各种恶性肿瘤患者的预后评估。然而,SIRI在宫颈癌患者中的预后价值尚未见报道。本研究发现,较高的SIRI与淋巴管浸润相关,也与国际妇产科联盟(FIGO)分期、放疗、中性粒细胞/淋巴细胞比值(NLR)、血小板/淋巴细胞比值(PLR)和单核细胞/淋巴细胞比值(MLR)显著相关,但与其他临床和病理参数无关。根据Kaplan-Meier生存分析,高SIRI与原发性和验证组宫颈癌患者的不良预后相关。SIRI、NLR、PLR和MLR均可用于确定可手术宫颈癌患者的预后。此外,证实只有SIRI是可手术宫颈癌患者的独立预后因素。倾向评分匹配(PSM)分析也得到了相同的结果。在ROC曲线分析中,SIRI在预测宫颈癌患者预后方面更准确。然后,基于SIRI、FIGO分期和淋巴管浸润建立了列线图,其在确定宫颈癌患者预后方面比FIGO分期更准确。验证队列显示了相同的结果。此外,术后4-8周SIRI相对于基线值的变化与宫颈癌患者的生存密切相关。与SIRI无变化(变异绝对值<25%)的患者相比,SIRI升高>75%的宫颈癌患者总生存期较差(<0.001),而SIRI降低>75%的患者预后较好(<0.001)。SIRI可作为可治愈宫颈癌患者的新的独立预后指标和治疗反应监测的潜在标志物。与传统的FIGO分期系统相比,整合SIRI的列线图在根治性手术后能更客观、可靠地预测宫颈癌患者的生存情况。