Department of Clinical Microbiology, University College London, London, UK.
Hospital for Tropical Diseases, University College London, London, UK; Clinical Research Department, London School of Hygiene & Tropical Medicine, London, UK.
J Hosp Infect. 2020 Aug;105(4):632-637. doi: 10.1016/j.jhin.2020.05.035. Epub 2020 May 30.
The COVID-19 pandemic presents a significant infection prevention and control challenge. The admission of large numbers of patients with suspected COVID-19 disease risks overwhelming the capacity to protect other patients from exposure. The delay between clinical suspicion and confirmatory testing adds to the complexity of the problem.
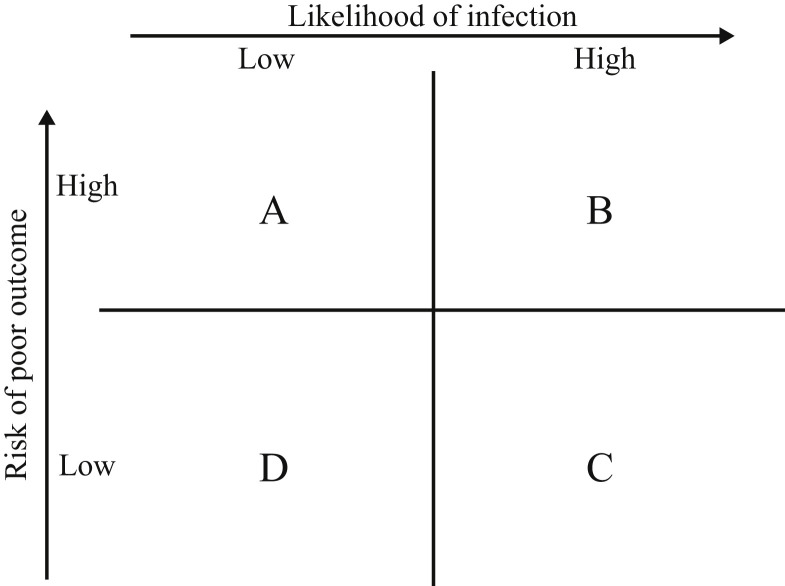
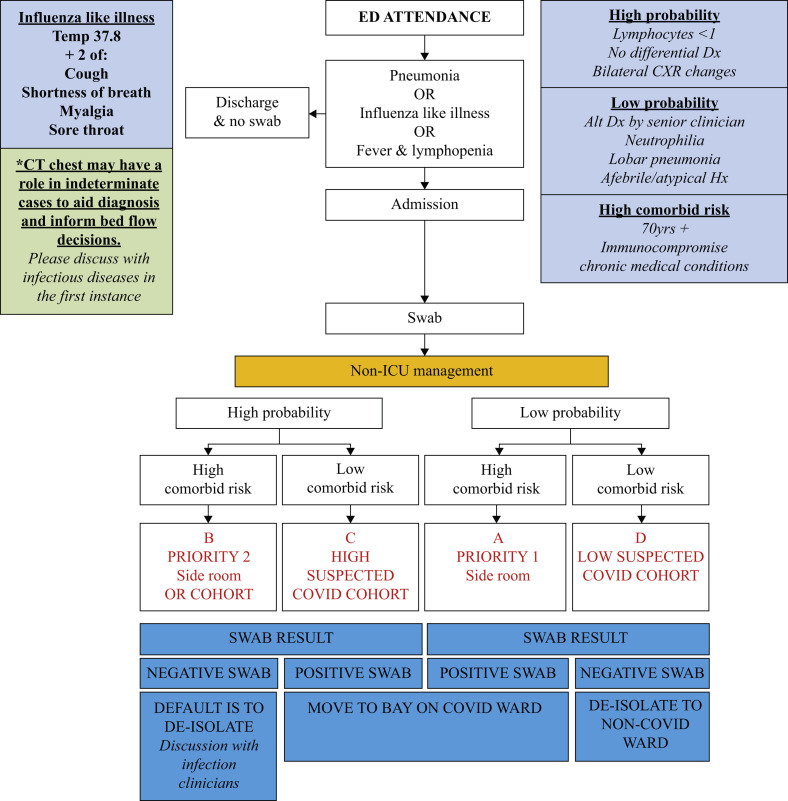
We implemented a triage tool aimed at minimizing hospital-acquired COVID-19 particularly in patients at risk of severe disease. Patients were allocated to triage categories defined by likelihood of COVID-19 and risk of a poor outcome. Category A (low-likelihood; high-risk), B (high-likelihood; high-risk), C (high-likelihood; low-risk) and D (low-likelihood; low-risk). This determined the order of priority for isolation in single-occupancy rooms with Category A the highest. Patients in other groups were cohorted when isolation capacity was limited with additional interventions to reduce transmission.
Ninety-three patients were evaluated with 79 (85%) receiving a COVID-19 diagnosis during their admission. Of those without a COVID-19 diagnosis: 10 were initially triaged to Category A; 0 to B; 1 to C and 4 to D. All high-risk patients requiring isolation were, therefore, admitted to single-occupancy rooms and protected from exposure. Twenty-eight (30%) suspected COVID-19 patients were evaluated to be low risk (groups C and D) and eligible for cohorting. No symptomatic hospital-acquired infections were detected in the cohorted patients.
Application of a clinical triage tool to guide isolation and cohorting decisions may reduce the risk of hospital-acquired transmission of COVID-19 especially to individuals at the greatest of risk of severe disease.
COVID-19 大流行带来了重大的感染预防和控制挑战。大量疑似 COVID-19 疾病患者的入院,使保护其他患者免受暴露的能力面临巨大压力。从临床怀疑到确诊检测的时间延迟增加了问题的复杂性。
我们实施了一种分诊工具,旨在最大限度地减少医院获得性 COVID-19,特别是在有发生严重疾病风险的患者中。根据 COVID-19 的可能性和不良结局的风险,将患者分配到分诊类别。A 类(低可能性;高风险)、B 类(高可能性;高风险)、C 类(高可能性;低风险)和 D 类(低可能性;低风险)。这决定了隔离的优先顺序,A 类最高。当隔离能力有限时,其他组的患者将被分组,同时采取额外的干预措施来减少传播。
93 名患者接受了评估,其中 79 名(85%)在入院期间被诊断为 COVID-19。在没有 COVID-19 诊断的患者中:10 例最初分诊为 A 类;0 例为 B 类;1 例为 C 类;4 例为 D 类。因此,所有需要隔离的高风险患者都被收治到单人病房,免受感染。28 例(30%)疑似 COVID-19 患者被评估为低风险(C 类和 D 类),符合分组条件。在分组患者中未发现有症状的医院获得性感染。
应用临床分诊工具来指导隔离和分组决策可能会降低医院获得性 COVID-19 传播的风险,特别是对那些有发生严重疾病最大风险的个体。