Zhang Zhonghan, Zhang Yang, Luo Fan, Ma Yuxiang, Fang Wenfeng, Zhan Jing, Li Su, Yang Yunpeng, Zhao Yuanyuan, Hong Shaodong, Zhou Ting, Zhang Yaxiong, Zhao Shen, Huang Yan, Zhao Hongyun, Zhang Li
Department of Medical Oncology, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, P. R. China.
Department of Clinical Research, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, P. R. China.
Clin Transl Med. 2020 Jun;10(2):e33. doi: 10.1002/ctm2.33. Epub 2020 Jun 4.
Dual blockade of both EGFR and VEGFR pathways in EGFR-mutant NSCLC have shown enhanced antitumor efficacy versus EGFR-TKIs alone. Apatinib is an orally effective VEGFR-2 tyrosine kinase inhibitor (TKI). This pilot study aims to evaluate the tolerability, pharmacokinetic profile, and antitumor activity of apatinib plus gefitinib as a therapy for EGFR-mutant advanced NSCLC.
Advanced non-squamous NSCLC participants harbored with the EGFR 19 deletion or the 21 L858R point mutation were included. There were two cohorts: Cohort A: apatinib 500 mg + gefitinib 250 mg. Cohort B: apatinib 250 mg + gefitinib 250 mg. The primary endpoint was safety profile. Other endpoints consisted of PK analysis, objective response rate (ORR), and progression-free survival (PFS). Exploratory analysis was conducted using next-generation sequencing of plasma circulating-tumor DNA.
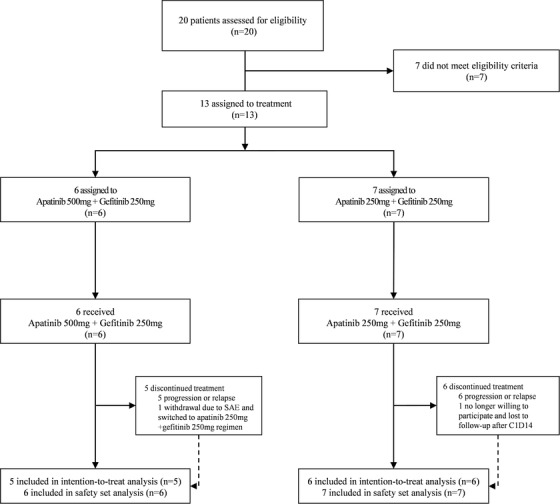
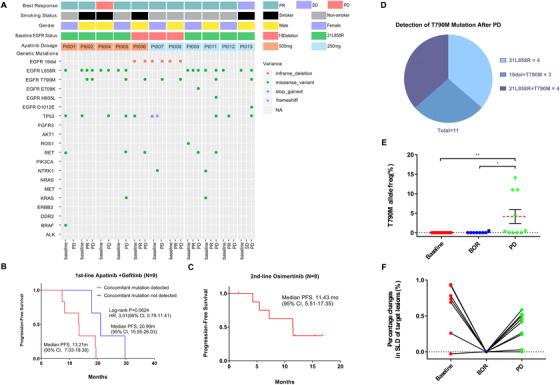
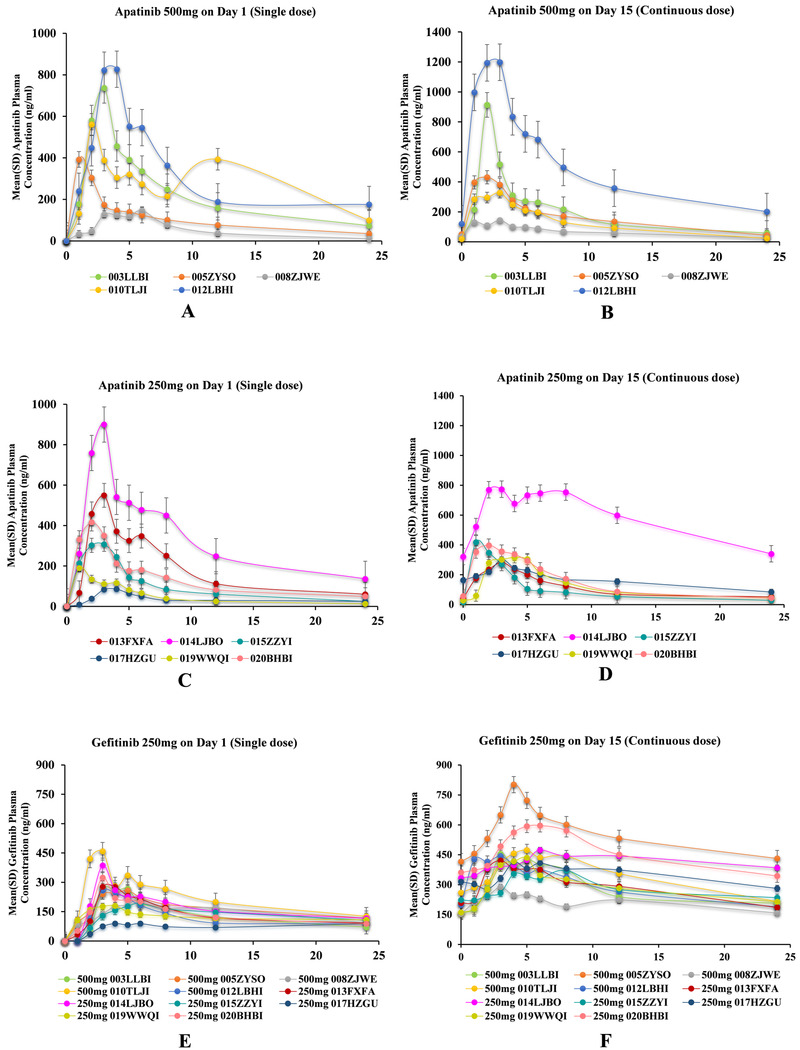
Between July 2016 and April 2017, 13 of NSCLC patients were recruited. Six patients were pooled in Cohort A, while seven patients were in Cohort B. Adverse events (AEs) were tolerable (mostly grade 1-2) and the treatment-related AEs were similar in both cohorts: rash (100% vs 71.4%), diarrhea (66.7% vs 71.4%), hypertension (66.7% vs 71.4%), proteinuria (66.7% vs 42.9%), and hand-foot skin reaction (33.3% vs 28.6%). The area under plasma concentration-time curve for the steady state of apatinib was 2864.73 ± 2605.54 ng mL h in Cohort A and 2445.09 ± 1550.89 ng mL h in Cohort B. Of the 11 patients evaluable for efficacy, Cohort A achieved an ORR of 80.0% and reached a median PFS of 19.2 months, while it was 83.3% and 13.4 months in Cohort B. Patients without a concomitant mutation at baseline had a prolonged PFS tendency (20.99 months v 13.21 months, P = .0624). The EGFR-T790M mutation remained the dominant resistance mechanism.
Apatinib (500 mg) plus gefitinib (250 mg) showed a tolerable safety profile and encouraging antitumor activity for advanced EGFR-mutant NSCLC in the first-line setting. Phase III trials of apatinib (500 mg) plus gefitinib (250 mg) are warranted.
Clinicaltrials.gov, NCT02824458, date of registration June 23, 2016.
在表皮生长因子受体(EGFR)突变的非小细胞肺癌(NSCLC)中,对EGFR和血管内皮生长因子受体(VEGFR)通路进行双重阻断已显示出相较于单独使用EGFR酪氨酸激酶抑制剂(TKI)更强的抗肿瘤疗效。阿帕替尼是一种口服有效的VEGFR-2酪氨酸激酶抑制剂。这项前瞻性研究旨在评估阿帕替尼联合吉非替尼治疗EGFR突变的晚期NSCLC的耐受性、药代动力学特征和抗肿瘤活性。
纳入患有EGFR 19外显子缺失或21 L858R点突变的晚期非鳞状NSCLC患者。有两个队列:队列A:阿帕替尼500毫克+吉非替尼250毫克。队列B:阿帕替尼250毫克+吉非替尼250毫克。主要终点是安全性。其他终点包括药代动力学分析、客观缓解率(ORR)和无进展生存期(PFS)。使用血浆循环肿瘤DNA的二代测序进行探索性分析。
2016年7月至2017年4月期间,招募了13例NSCLC患者。6例患者归入队列A,7例患者归入队列B。不良事件(AE)可耐受(大多为1-2级),且两个队列中与治疗相关的AE相似:皮疹(100%对71.4%)、腹泻(66.7%对71.4%)、高血压(66.7%对71.4%)、蛋白尿(66.7%对42.9%)和手足皮肤反应(33.3%对28.6%)。队列A中阿帕替尼稳态时的血浆浓度-时间曲线下面积为2864.73±2605.54纳克·毫升·小时,队列B中为2445.09±1550.89纳克·毫升·小时。在11例可评估疗效的患者中,队列A的ORR为80.0%,中位PFS达到19.2个月,而队列B中分别为83.3%和13.4个月。基线时无伴随突变的患者有PFS延长的趋势(20.99个月对13.21个月,P = 0.0624)。EGFR-T790M突变仍然是主要的耐药机制。
阿帕替尼(500毫克)联合吉非替尼(250毫克)在一线治疗晚期EGFR突变的NSCLC中显示出可耐受的安全性和令人鼓舞的抗肿瘤活性。有必要开展阿帕替尼(500毫克)联合吉非替尼(250毫克)的III期试验。
Clinicaltrials.gov,NCT02824458,注册日期2016年6月23日。