Tang Fan, Tie Yan, Tu Chongqi, Wei Xiawei
State Key Laboratory of Biotherapy and Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People's Republic of China.
Department of Orthopeadics, West China Hospital, Sichuan University, Chengdu, Sichuan, People's Republic of China.
Clin Transl Med. 2020 Jan;10(1):199-223. doi: 10.1002/ctm2.24.
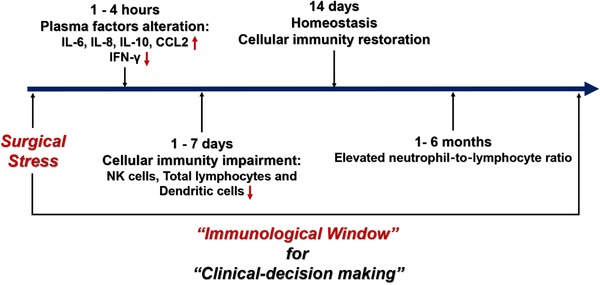
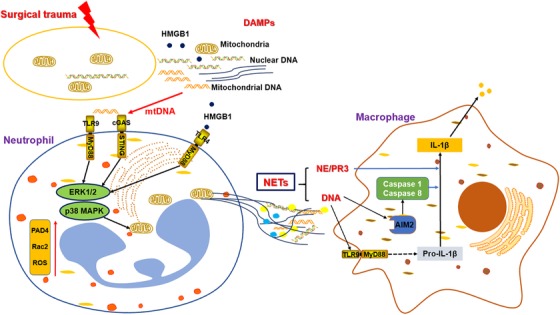
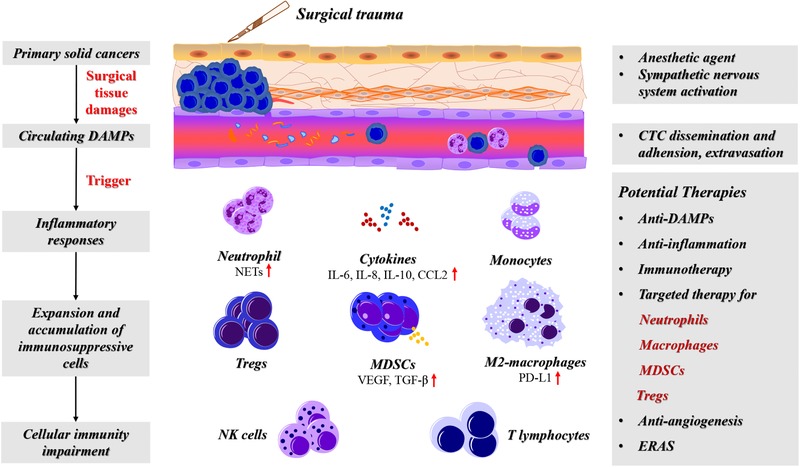
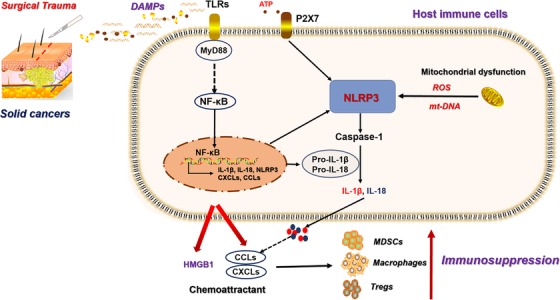
Surgical resection remains the mainstay treatment for solid cancers, especially for localized disease. However, the postoperative immunosuppression provides a window for cancer cell proliferation and awakening dormant cancer cells, leading to rapid recurrences or metastases. This immunosuppressive status after surgery is associated with the severity of surgical trauma since immunosuppression induced by minimally invasive surgery is less than that of an extensive open surgery. The systemic response to tissue damages caused by surgical operations and the subsequent wound healing induced a cascade alteration in cellular immunity. After surgery, patients have a high level of circulating damage-associated molecular patterns (DAMPs), triggering a local and systemic inflammation. The inflammatory metrics in the immediate postoperative period was associated with the prognosis of cancer patients. Neutrophils provide the first response to surgical trauma, and the production of neutrophil extracellular traps (NETs) promotes cancer progression. Activated macrophage during wound healing presents a tumor-associated phenotype that cancers can exploit for their survival advantage. In addition, the amplification and activation of myeloid-derived suppressor cells (MDSCs), regulatory T cells (Tregs) or the elevated programmed death ligand-1 and vascular endothelial growth factor expression under surgical trauma, exacerbate the immunosuppression and favor of the formation of the premetastatic niche. Therapeutic strategies to reduce the cellular immunity impairment after surgery include anti-DAMPs, anti-postoperative inflammation or inflammatory/pyroptosis signal, combined immunotherapy with surgery, antiangiogenesis and targeted therapies for neutrophils, macrophages, MDSCs, and Tregs. Further, the application of enhanced recovery after surgery also has a feasible outcome for postoperative immunity restoration. Overall, current therapies to improve the cellular immunity under the special condition after surgery are relatively lacking. Further understanding the underlying mechanisms of surgical trauma-related immunity dysfunction, phenotyping the immunosuppressive cells, and developing the related therapeutic intervention should be explored.
手术切除仍然是实体癌的主要治疗方法,尤其是对于局限性疾病。然而,术后免疫抑制为癌细胞增殖和唤醒休眠癌细胞提供了一个窗口,导致快速复发或转移。手术后的这种免疫抑制状态与手术创伤的严重程度相关,因为微创手术诱导的免疫抑制小于广泛开放手术。机体对手术操作引起的组织损伤及随后伤口愈合的反应导致细胞免疫发生一系列改变。手术后,患者循环中的损伤相关分子模式(DAMPs)水平较高,引发局部和全身炎症。术后即刻的炎症指标与癌症患者的预后相关。中性粒细胞对手术创伤产生第一反应,中性粒细胞胞外陷阱(NETs)的产生促进癌症进展。伤口愈合过程中活化的巨噬细胞呈现肿瘤相关表型,癌症可利用这种表型获得生存优势。此外,手术创伤下髓源性抑制细胞(MDSCs)、调节性T细胞(Tregs)的扩增和激活,或程序性死亡配体-1和血管内皮生长因子表达升高,会加剧免疫抑制并有利于前转移微环境的形成。减轻术后细胞免疫损伤的治疗策略包括抗DAMPs、抗术后炎症或炎症/焦亡信号、手术联合免疫治疗、抗血管生成以及针对中性粒细胞、巨噬细胞、MDSCs和Tregs的靶向治疗。此外,术后加速康复的应用对于术后免疫恢复也有可行的效果。总体而言,目前在手术后特殊情况下改善细胞免疫的治疗方法相对缺乏。应进一步探索手术创伤相关免疫功能障碍的潜在机制、对免疫抑制细胞进行表型分析以及开发相关治疗干预措施。