Department of Medicine, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania.
Department of Medicine, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania.
Heart Rhythm. 2020 Sep;17(9):1434-1438. doi: 10.1016/j.hrthm.2020.06.009. Epub 2020 Jun 11.
Myriad manifestations of cardiovascular involvement have been described in patients with coronavirus disease 2019 (COVID-19), but there have been no reports of COVID-19 affecting the cardiac conduction system. The PR interval on the electrocardiogram (ECG) normally shortens with increasing heart rate (HR). The case of a patient with COVID-19 manifesting Mobitz type 1 atrioventricular (AV) block that normalized as the patient's condition improved prompted us to investigate PR interval behavior in patients with COVID-19.
The purpose of this study was to characterize PR interval behavior in hospitalized patients with COVID-19 and to correlate that behavior with clinical outcomes.
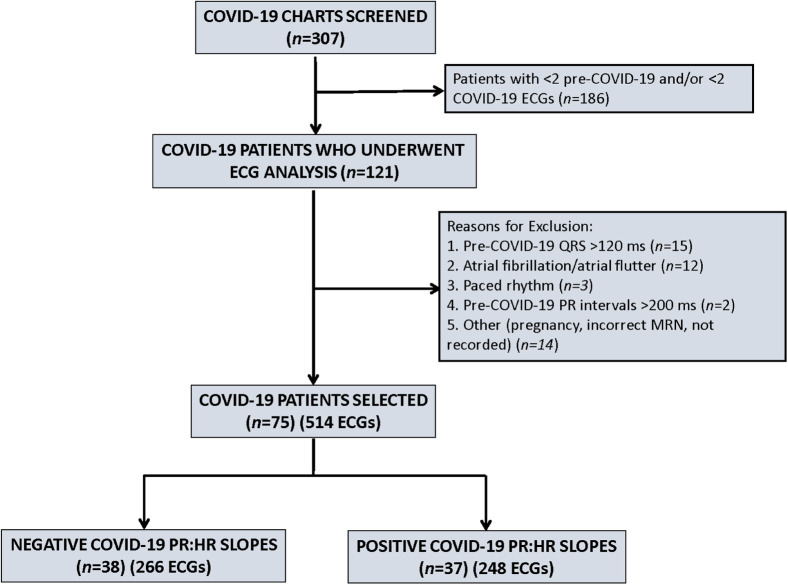
This study was a cross-sectional cohort analysis of confirmed COVID-19 cases (March 26, 2020, to April 25, 2020). We reviewed pre-COVID-19 and COVID-19 ECGs to characterize AV conduction by calculating the PR interval to HR (PR:HR) slope. Clinical endpoints were death or need for endotracheal intubation.
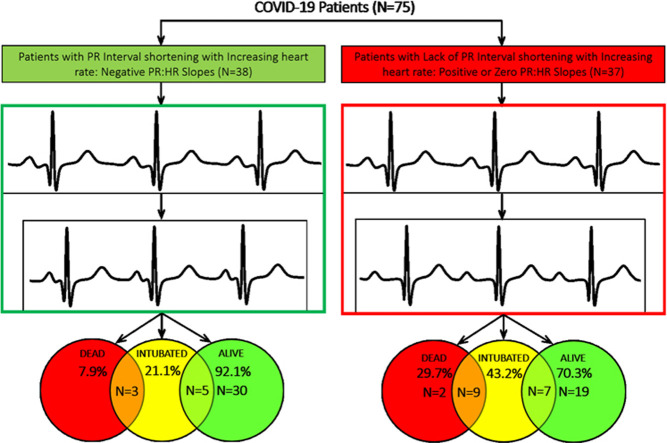
ECGs from 75 patients (246 pre-COVID-19 ECGs and 246 COVID-19 ECGs) were analyzed for PR:HR slope. Of these patients, 38 (50.7%) showed the expected PR interval shortening with increasing HR (negative PR:HR slope), whereas 37 (49.3%) showed either no change (8 with PR:HR slope = 0) or paradoxical PR interval prolongation (29 with positive PR:HR slope) with increasing HR. Patients without PR interval shortening were more likely to die (11/37 [29.7%] vs 3/38 [7.9%]; P = .019) or require endotracheal intubation (16/37 [43.2%] vs 8/38 [21.1%]; P = .05) compared to patients with PR interval shortening.
Half of patients with COVID-19 showed abnormal PR interval behavior (paradoxical prolongation or lack of shortening) with increasing HR. This finding was associated with increased risk of death and need for endotracheal intubation.
在新冠肺炎(COVID-19)患者中,已经描述了心血管受累的多种表现,但尚未有报道称 COVID-19 会影响心脏传导系统。心电图(ECG)的 PR 间期通常随着心率(HR)的增加而缩短。我们报道了一例 COVID-19 患者表现出莫氏Ⅰ型房室(AV)阻滞,随着病情的改善而恢复正常,这促使我们研究 COVID-19 患者的 PR 间期行为。
本研究旨在描述住院 COVID-19 患者的 PR 间期行为,并将其与临床结局相关联。
这是一项横断面队列分析研究,纳入了 2020 年 3 月 26 日至 4 月 25 日期间确诊的 COVID-19 病例。我们回顾了 COVID-19 之前和 COVID-19 期间的心电图,通过计算 PR 间期与 HR(PR:HR)斜率来描述 AV 传导。临床终点为死亡或需要气管插管。
对 75 例患者(246 份 COVID-19 之前的心电图和 246 份 COVID-19 期间的心电图)的 PR:HR 斜率进行了分析。其中,38 例(50.7%)表现出与预期相符的 PR 间期随 HR 增加而缩短(PR:HR 斜率为负),而 37 例(49.3%)表现为 PR 间期无变化(8 例 PR:HR 斜率=0)或随 HR 增加而出现矛盾的 PR 间期延长(29 例 PR:HR 斜率为正)。没有 PR 间期缩短的患者更有可能死亡(37/37 [29.7%] vs 38/38 [7.9%];P=0.019)或需要气管插管(37/37 [43.2%] vs 38/38 [21.1%];P=0.05)。
一半的 COVID-19 患者表现出异常的 PR 间期行为(矛盾的延长或无缩短),随 HR 增加而出现。这一发现与死亡和需要气管插管的风险增加相关。