Yamaguchi Hayato, Fukuzawa Masakatsu, Minami Hirohito, Ichimiya Tadashi, Takahashi Hiroshi, Matsue Yubu, Honjo Mitsuyoshi, Hirayama Yasutake, Nutahara Daisuke, Taira Junichi, Nakamura Hironori, Kawai Takashi, Itoi Takao
Department of Gastroenterology and Hepatology, Tokyo Medical University Hachioji Medical Center, Japan.
Department of Gastroenterology and Hepatology, Tokyo Medical University, Japan.
Intern Med. 2020;59(12):1481-1488. doi: 10.2169/internalmedicine.4212-19. Epub 2020 Jun 15.
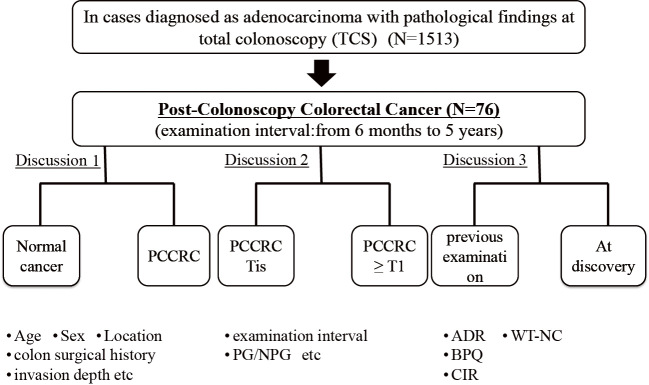
Objective This study aims to elucidate the association between the clinical characteristics of post-colonoscopy colorectal cancer (PCCRC) and quality indicators (QIs) of colonoscopy. Methods Patients with PCCRC who underwent total colonoscopy (TCS) and were histologically diagnosed with adenocarcinoma within six months to five years of the last examination were included in this study. PCCRC and normally detected cancer (NDC) identified within the same period were compared in terms of their clinicopathological characteristics. Furthermore, the QIs at PCCRC detection were compared to those at the last examination. Results Patients with PCCRC had a significantly higher rate of colon surgery history than those with NDC (PCCRC: 25/76, 32.9%; NDC: 31/1,437, 2.2%; p<0.001), but the invasion depth in these patients was significantly shallower (PCCRC: ≤Tis/≥T1, 37/39; NDC: ≤Tis/≥T1, 416/1,021; p<0.001). Among patients with PCCRC, the T1b group had significantly more non-polypoid growth (NPG)-type cases than PG-type CRC cases (p=0.018). The adenoma detection rate (ADR) of colonoscopists performing TCS was 30.2-52.8%. Furthermore, the ADR of colonoscopists at the time of PCCRC detection (36.7%±5.9%) was significantly higher than that of colonoscopists who performed the last examination (34.9%±4.4%; p=0.034). The withdrawal time for negative colonoscopy (WT-NC) at detection was significantly longer than that at the last examination (at detection: 494.3±253.8 s; at last examination: 579.5±243.6 s; p=0.010). Conclusion Given that these PCCRC cases were post-colon surgery cases, had a long WT-NC, and were detected by colonoscopists with a high ADR, most cases showed lesions that were missed during the previous colonoscopy. Caution should be practiced in order to avoid missing flat, NPG-type tumors.
目的 本研究旨在阐明结肠镜检查后结直肠癌(PCCRC)的临床特征与结肠镜检查质量指标(QIs)之间的关联。方法 本研究纳入了接受全结肠镜检查(TCS)且在最后一次检查后6个月至5年内经组织学诊断为腺癌的PCCRC患者。比较PCCRC患者与同期发现的正常检测到的癌症(NDC)患者的临床病理特征。此外,比较PCCRC检测时与最后一次检查时的QIs。结果 PCCRC患者的结肠手术史发生率显著高于NDC患者(PCCRC:25/76,32.9%;NDC:31/1437,2.2%;p<0.001),但这些患者的浸润深度明显更浅(PCCRC:≤Tis/≥T1,37/39;NDC:≤Tis/≥T1,416/1021;p<0.001)。在PCCRC患者中,T1b组的非息肉样生长(NPG)型病例明显多于息肉样结直肠癌(PG型CRC)病例(p=0.018)。进行TCS的结肠镜检查医师的腺瘤检出率(ADR)为30.2 - 52.8%。此外,PCCRC检测时结肠镜检查医师的ADR(36.7%±5.9%)显著高于进行最后一次检查的结肠镜检查医师(34.9%±4.4%;p=0.034)。检测时结肠镜检查阴性的退镜时间(WT-NC)显著长于最后一次检查时(检测时:494.3±253.8秒;最后一次检查时:579.5±243.6秒;p=0.010)。结论 鉴于这些PCCRC病例为结肠手术后病例,WT-NC时间长,且由ADR高的结肠镜检查医师检测到,大多数病例显示出在前次结肠镜检查时漏诊的病变。应谨慎操作以避免漏诊扁平的NPG型肿瘤。