Department of Medical Oncology, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
Department of Oncology, Henan Cancer Hospital, The Affiliated Cancer Hospital of Zhengzhou University, Zhengzhou, China.
Front Immunol. 2020 May 28;11:1037. doi: 10.3389/fimmu.2020.01037. eCollection 2020.
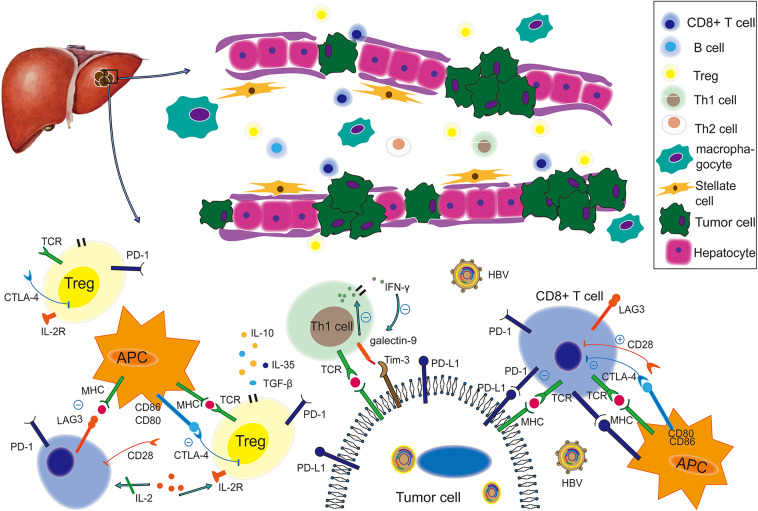
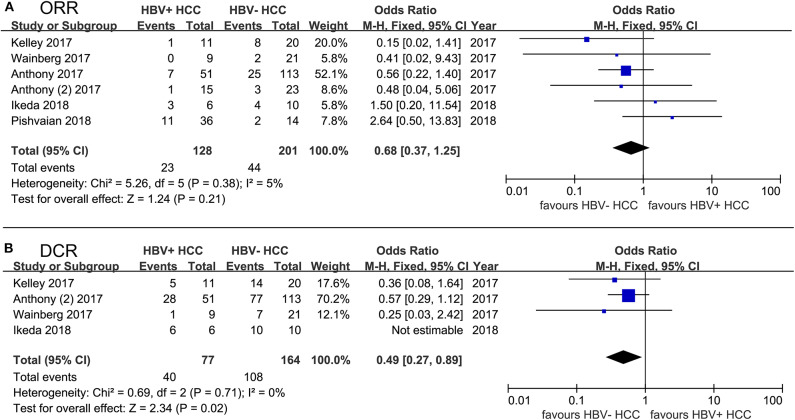
Hepatitis B virus (HBV) infection is regarded as the main etiological risk factor in the process of hepatocellular carcinoma (HCC), as it promotes an immunosuppressive microenvironment that is partially mediated by the programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) signaling pathway. The tumor microenvironment (TME) of HBV-related HCC is indeed more immunosuppressive than microenvironments not associated with viruses. And compared to TME in hepatitis C virus (HCV) infected HCC, TME of HBV-related HCC is less vascularized and presents different immune components resulting in similar immunosuppression. However, few studies are focusing on the specific side effects and efficacy of PD-1/PD-L1 blockade immunotherapy in HBV-related HCC patients, as well as on the underlying mechanism. Herein, we reviewed the basic research focusing on potential TME alteration caused by HBV infection, especially in HCC patients. Moreover, we reviewed PD-1/PD-L1 blockade immunotherapy clinical trials to clarify the safety and efficacy of this newly developed treatment in the particular circumstances of HBV infection. We found that patients with HBV-related HCC displayed an acceptable safety profile similar to those of non-infected HCC patients. However, we could not determine the antiviral activity of PD-1/PD-L1 blockade because standard anti-viral therapies were conducted in all of the current clinical trials, which made it difficult to distinguish the potential influence of PD-1/PD-L1 blockade on HBV infection. Generally, the objective response rates (ORRs) of PD-1/PD-L1 blockade immunotherapy did not differ significantly between virus-positive and virus-negative patients, except that disease control rates (DCRs) were obviously lower in HBV-infected HCC patients.
乙型肝炎病毒(HBV)感染被认为是肝细胞癌(HCC)发生过程中的主要病因学风险因素,因为它促进了部分由程序性细胞死亡蛋白 1(PD-1)/程序性死亡配体 1(PD-L1)信号通路介导的免疫抑制微环境。HBV 相关 HCC 的肿瘤微环境(TME)确实比与病毒无关的微环境具有更强的免疫抑制性。与丙型肝炎病毒(HCV)感染相关 HCC 的 TME 相比,HBV 相关 HCC 的 TME 血管化程度较低,并且具有不同的免疫成分,导致类似的免疫抑制。然而,很少有研究关注 PD-1/PD-L1 阻断免疫疗法在 HBV 相关 HCC 患者中的具体副作用和疗效,以及潜在机制。在这里,我们回顾了专注于 HBV 感染引起的潜在 TME 改变的基础研究,特别是在 HCC 患者中。此外,我们还回顾了 PD-1/PD-L1 阻断免疫疗法的临床试验,以阐明这种新开发的治疗方法在 HBV 感染特殊情况下的安全性和疗效。我们发现,HBV 相关 HCC 患者的安全性与未感染 HCC 患者相似。然而,我们无法确定 PD-1/PD-L1 阻断的抗病毒活性,因为目前所有临床试验均进行了标准抗病毒治疗,这使得难以区分 PD-1/PD-L1 阻断对 HBV 感染的潜在影响。一般来说,PD-1/PD-L1 阻断免疫疗法的客观缓解率(ORR)在病毒阳性和病毒阴性患者之间没有显著差异,除了 HBV 感染 HCC 患者的疾病控制率(DCR)明显较低。