Department Medical Sciences, Infectious Diseases and Dermatology Section, University of Ferrara, Italy.
Dept. Morphology, Surgery, Exp. Medicine, PhDs Molecular Medicine, University of Ferrara, Italy.
Med Hypotheses. 2020 Nov;144:109876. doi: 10.1016/j.mehy.2020.109876. Epub 2020 May 24.
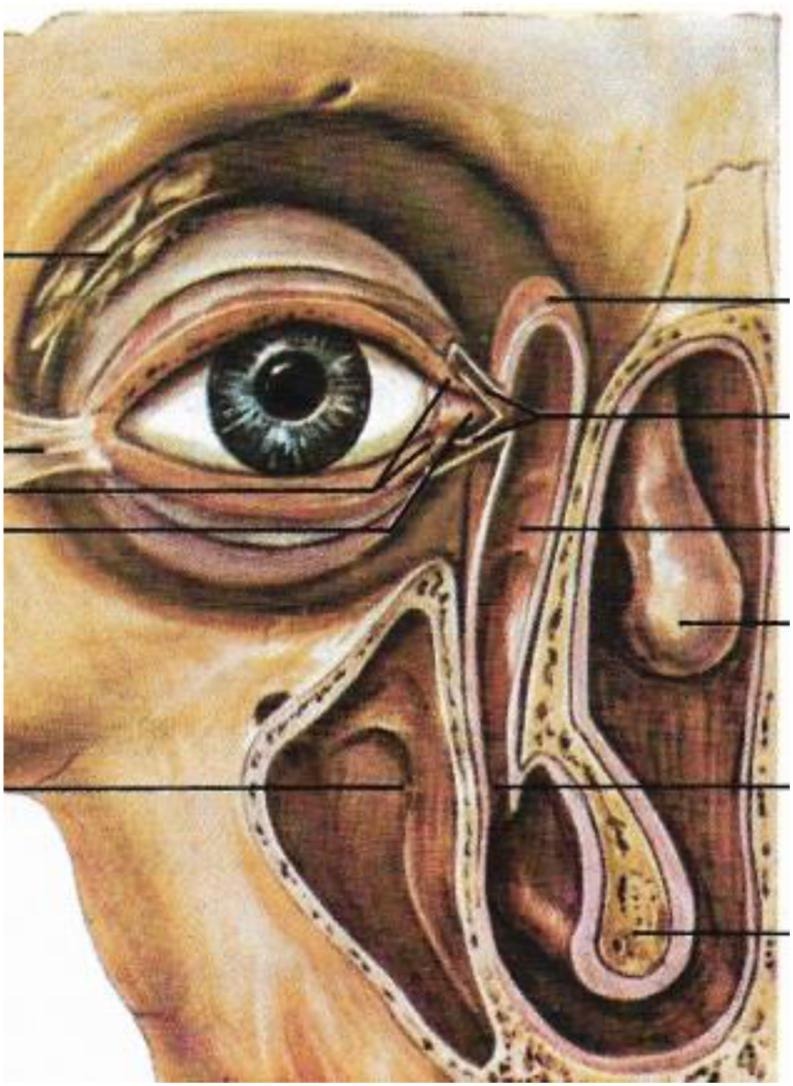
The new zoonotic coronavirus (SARS-CoV-2) responsible for coronavirus disease (COVID-19) is a new strain of coronavirus not previously seen in humans and which appears to come from bat species. It originated in Wuhan, Hubei Province, China, and spread rapidly throughout the world, causing over 5,569,679 global cases and 351,866 deaths in almost every country in the world, including Europe, particularly Italy. In general, based on existing data published to date, 80.9% of patients infected with the virus develop mild infection; 13.8% severe pneumonia; 4.7% respiratory failure, septic shock or multi-organ failure; 3% of these cases are fatal. Critical patients have been shown to develop acute respiratory distress syndrome (ARDS) and hospitalization in intensive care units. The average age of patients admitted to hospital is 57-79 years, with one third half with an underlying disease. Asymptomatic infections have also been described, but their frequency is not known. SARS-CoV-2 transmission is mainly airborne from one person to another via droplets. The data available so far seem to indicate that SARS-CoV-2 is capable of producing an excessive immune reaction in the host. The virus attacks type II pneumocytes in the lower bronchi through the binding of the Spike protein (S protein) to viral receptors, of which the angiotensin 2 conversion enzyme (ACE2) receptor is the most important. ACE2 receptor is widely expressed in numerous tissues, including the oropharynx and conjunctiva, but mostly distributed in ciliated bronchial epithelial cells and type II pneumocytes in the lower bronchi. The arrival of SARS-CoV-2 in the lungs causes severe primary interstitial viral pneumonia that can lead to the "cytokine storm syndrome", a deadly uncontrolled systemic inflammatory response triggered by the activation of interleukin 6 (IL-6), whose effect is extensive lung tissue damage and disseminated intravascular coagulation (DIC), that are life-threatening for patients with COVID-19. In the absence of a therapy of proven efficacy, current management consists of off-label or compassionate use therapies based on antivirals, antiparasitic agents in both oral and parenteral formulation, anti-inflammatory drugs, oxygen therapy and heparin support and convalescent plasma. Like most respiratory viruses can function and replicate at low temperatures (i.e. 34-35 °C) and assuming viral thermolability of SARS-CoV-2, local instillation or aerosol of antiviral (i.e. remdesivir) in humid heat vaporization (40°-41 °C) in the first phase of infection (phenotype I, before admission), both in asymptomatic but nasopharyngeal swab positive patients, together with antiseptic-antiviral oral gargles and povidone-iodine eye drops for conjunctiva (0,8-5% conjunctival congestion), would attack the virus directly through the receptors to which it binds, significantly decreasing viral replication, risk of evolution to phenotypes IV and V, reducing hospitalization and therefore death.
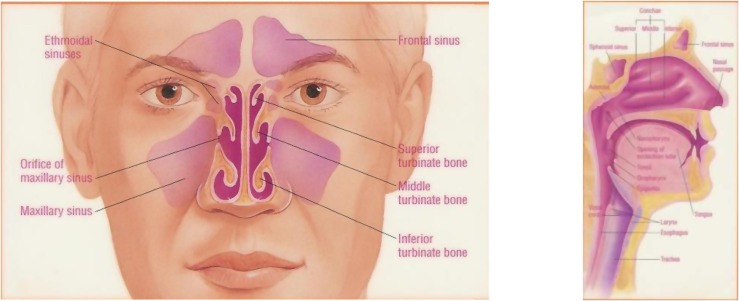
新型人畜共患冠状病毒(SARS-CoV-2)是一种以前未在人类中发现的新型冠状病毒,似乎来自蝙蝠物种。它起源于中国湖北省武汉市,迅速在全球范围内传播,导致全球超过 5569679 例病例和 351866 例死亡,几乎包括欧洲在内的世界上每个国家都受到了影响,尤其是意大利。一般来说,根据迄今为止已发表的现有数据,80.9%的病毒感染者为轻症感染;13.8%为重症肺炎;4.7%为呼吸衰竭、感染性休克或多器官衰竭;这些病例中有 3%是致命的。重症患者会出现急性呼吸窘迫综合征(ARDS)并需要住院重症监护治疗。住院患者的平均年龄为 57-79 岁,三分之一有基础疾病。也有描述无症状感染,但不知道其频率。SARS-CoV-2 的传播主要是人与人之间通过飞沫空气传播。到目前为止的数据似乎表明,SARS-CoV-2 能够在宿主中产生过度的免疫反应。病毒通过 Spike 蛋白(S 蛋白)与病毒受体结合,攻击下支气管中的 II 型肺泡细胞,其中血管紧张素 2 转换酶(ACE2)受体是最重要的。ACE2 受体在许多组织中广泛表达,包括口咽和结膜,但主要分布在有纤毛的支气管上皮细胞和下支气管的 II 型肺泡细胞中。SARS-CoV-2 到达肺部会导致严重的原发性间质病毒性肺炎,从而导致“细胞因子风暴综合征”,这是一种由白细胞介素 6(IL-6)激活引发的致命性、不受控制的全身炎症反应,其作用是广泛的肺组织损伤和弥散性血管内凝血(DIC),这对 COVID-19 患者是生命威胁。在没有经过证实疗效的治疗方法的情况下,目前的治疗方法包括基于抗病毒药物的标签外或同情用药治疗、口服和肠胃外制剂的抗寄生虫药物、抗炎药物、氧疗和肝素支持以及恢复期血浆。像大多数呼吸道病毒一样,SARS-CoV-2 可以在低温下(即 34-35°C)发挥功能和复制,并假设 SARS-CoV-2 的病毒热不稳定性,在感染的第一阶段(表型 I,入院前),对无症状但鼻咽拭子阳性的患者进行局部滴注或雾化抗病毒(即瑞德西韦)治疗,同时进行消毒抗病毒口腔漱口和聚维酮碘滴眼液治疗结膜(0.8-5%结膜充血),直接通过病毒结合的受体攻击病毒,显著降低病毒复制,降低向表型 IV 和 V 演变的风险,减少住院和死亡。