Department of Obstetrics and Gynaecology, Monash University, Melbourne, Australia.
MMGH Consulting, Zurich, Switzerland.
Vaccine. 2020 Jul 14;38(33):5268-5277. doi: 10.1016/j.vaccine.2020.05.084. Epub 2020 Jun 22.
To examine the characteristics of existing maternal tetanus immunization programmes for pregnant women in low- and middle-income countries (LMICs) and to identify and understand the challenges, barriers and facilitators associated with maternal vaccine service delivery that may impact the introduction and implementation of new maternal vaccines in the future.
A mixed methods, cross sectional study with four data collection phases including a desk review, online survey, telephone and face-to-face interviews and in country visits.
LMICs.
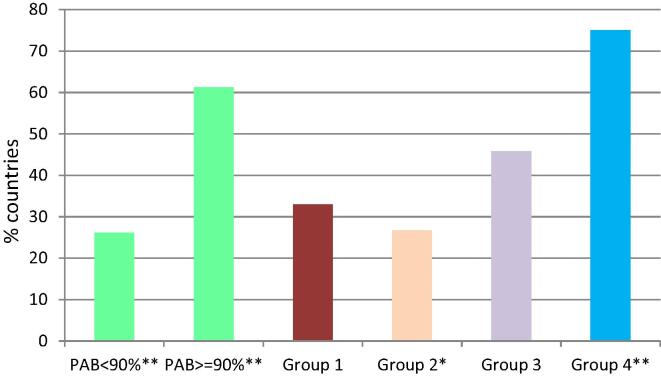
The majority of countries (84/95; 88%) had a maternal tetanus immunization policy. Countries with high protection at birth (PAB) were more likely to report tetanus toxoid-containing vaccine (TTCV) coverage targets > 90%. Less than half the countries included in this study had a TTCV coverage target of > 90%. Procurement and distribution of TTCV was nearly always the responsibility of the Expanded Programme on Immunization (EPI), however planning and management of maternal immunization was often shared between EPI and Maternal, Newborn and Child Health (MNCH) programmes. Receipt of TTCV at the same time as the antenatal care visit correlated with high PAB. Most countries (81/95; 85%) had an immunization safety surveillance system in place although only 11% could differentiate an adverse event following immunization (AEFI) in pregnant and non-pregnant women.
Recommendations arising from the MIACSA project to strengthen existing services currently delivering maternal tetanus immunization in LMICs include establishing and maintaining vaccination targets, clearly defining responsibilities and fostering collaborations between EPI and MNCH, investing in strengthening the health workforce, improving the design and use of existing record keeping for immunization, adjusting current AEFI reporting to differentiate pregnant women and endeavoring to integrate the provision of TTCV within ANC services where appropriate.
检查中低收入国家(LMIC)孕妇破伤风免疫接种规划的现有特点,并确定和了解与孕产妇疫苗接种服务提供相关的挑战、障碍和促进因素,这些因素可能会影响未来新的孕产妇疫苗的引入和实施。
一项混合方法、横断面研究,分为四个数据收集阶段,包括桌面审查、在线调查、电话和面对面访谈以及国家访问。
中低收入国家。
大多数国家(84/95;88%)都有破伤风免疫接种政策。在出生时具有高保护率(PAB)的国家更有可能报告破伤风类毒素疫苗(TTCV)覆盖率目标>90%。在这项研究中,只有不到一半的国家有 TTCV 覆盖率目标>90%。TTCV 的采购和分配几乎总是扩大免疫规划(EPI)的责任,但孕产妇免疫规划的计划和管理通常由 EPI 和孕产妇、新生儿和儿童健康(MNCH)方案共同承担。在接受产前保健访问的同时接种 TTCV 与高 PAB 相关。大多数国家(81/95;85%)都有免疫安全监测系统,但只有 11%的国家能够区分孕妇和非孕妇接种后的不良反应事件(AEFI)。
MIACSA 项目提出的加强中低收入国家现有服务以提供破伤风免疫接种的建议包括:建立和维持疫苗接种目标、明确界定责任以及促进 EPI 和 MNCH 之间的合作、投资加强卫生人力、改进现有免疫记录的设计和使用、调整当前 AEFI 报告以区分孕妇,并努力在适当情况下将 TTCV 的提供纳入 ANC 服务。