Yang Yingying, Chen Weiqi, Pan Yuesong, Yan Hongyi, Meng Xia, Liu Liping, Wang Yongjun, Wang Yilong
Department of Neurology, China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, China.
Front Neurol. 2020 Jun 10;11:534. doi: 10.3389/fneur.2020.00534. eCollection 2020.
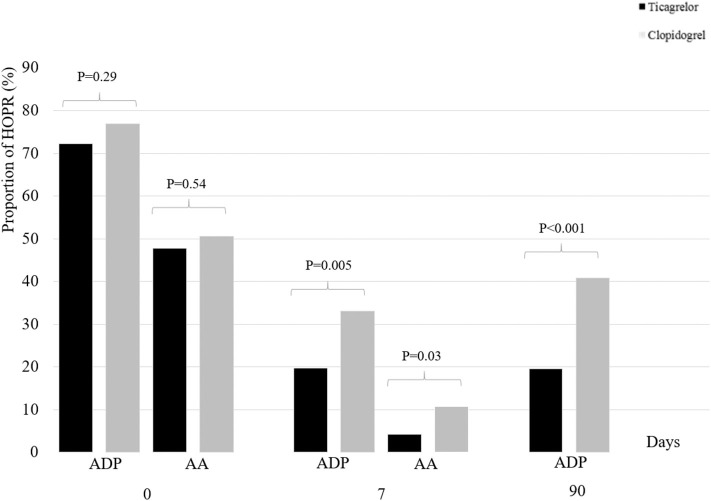
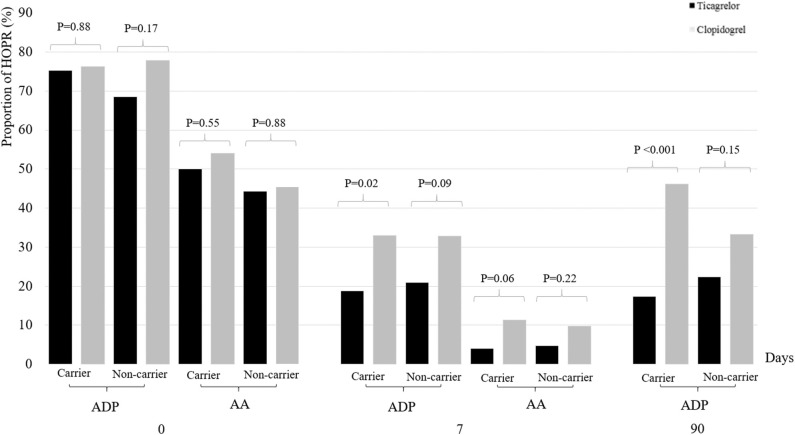
The combination of clopidogrel and aspirin is recommended for the treatment of patients with acute minor stroke or transient ischemic attack (TIA). However, with varied clopidogrel resistance (often due to loss-of-function (LOF) alleles), alternatives like ticagrelor have been suggested. Previous studies showed that ticagrelor had a lower platelet reactivity assessed by VerifyNow P2Y12 assay than clopidogrel. We aimed to compare the effect of ticagrelor vs. clopidogrel on platelet reactivity assessed by a different method (Aggrestar platelet function analyzer) and analyze whether genotypes were involved. A pre-specified subgroup analysis of a randomized controlled trial- Platelet Reactivity in Acute Non-disabling Cerebrovascular Events (PRINCE) was conducted. Patients with minor stroke or TIA were randomized for treatment with ticagrelor plus aspirin or clopidogrel plus aspirin. Platelet reactivity was assessed by Aggrestar (PL) platelet function analyzer and high on-treatment platelet reactivity (HOPR) on ticagrelor or clopidogrel was compared. Clinical outcomes included any stroke, composite vascular events and bleeding events within 90 days. Patients were categorized into carriers and non-carriers according to the carrier status of LOF alleles. Among 675 patients enrolled in the PRINCE trial, 387 patients were included in this subgroup: 197 were randomized to ticagrelor plus aspirin and 190 to clopidogrel plus aspirin. At 90 ± 7 days, compared with clopidogrel/aspirin group, the proportion of HOPR in ticagrelor/aspirin group was significantly lower (19.6 vs. 40.8%, < 0.001). No significant treatment-by-genotype interactions were found ( for interaction = 0.12). Within 90 days, a trend toward a lower risk of new stroke in ticagrelor/aspirin compared to clopidogrel/aspirin was observed (4.6 vs. 9.5%, HR 0.47, 95% CI 0.21-1.05, = 0.06). Ticagrelor is superior to clopidogrel in inhibiting platelet reactivity measured by the PL platelet function analyzer among patients with acute minor stroke or TIA. Our study confirmed the finding of the main analysis of PRINCE trial in a different assay. Large randomized controlled trials are needed to evaluate our findings. Clinicaltrials.gov NCT02506140.
氯吡格雷与阿司匹林联合用药被推荐用于治疗急性轻度卒中或短暂性脑缺血发作(TIA)患者。然而,由于氯吡格雷抵抗情况各异(常因功能丧失(LOF)等位基因所致),有人提出了替格瑞洛等替代药物。既往研究表明,通过VerifyNow P2Y12分析评估,替格瑞洛的血小板反应性低于氯吡格雷。我们旨在比较替格瑞洛与氯吡格雷对通过不同方法(Aggrestar血小板功能分析仪)评估的血小板反应性的影响,并分析是否涉及基因型因素。我们对一项随机对照试验——急性非致残性脑血管事件中的血小板反应性(PRINCE)进行了预先指定的亚组分析。轻度卒中和TIA患者被随机分为接受替格瑞洛加阿司匹林或氯吡格雷加阿司匹林治疗。通过Aggrestar(PL)血小板功能分析仪评估血小板反应性,并比较替格瑞洛或氯吡格雷治疗时的高治疗期血小板反应性(HOPR)。临床结局包括90天内的任何卒中、复合血管事件和出血事件。根据LOF等位基因的携带状态将患者分为携带者和非携带者。在PRINCE试验纳入的675例患者中,387例患者被纳入该亚组:197例被随机分配至替格瑞洛加阿司匹林组,190例被随机分配至氯吡格雷加阿司匹林组。在90±7天时,与氯吡格雷/阿司匹林组相比,替格瑞洛/阿司匹林组的HOPR比例显著更低(19.6%对40.8%,P<0.001)。未发现显著的治疗与基因型交互作用(交互作用P = 0.12)。在90天内,观察到与氯吡格雷/阿司匹林组相比,替格瑞洛/阿司匹林组新发卒中风险有降低趋势(4.6%对9.5%,风险比0.47,95%置信区间0.21 - 1.05,P = 0.06)。在急性轻度卒中和TIA患者中,通过PL血小板功能分析仪测量,替格瑞洛在抑制血小板反应性方面优于氯吡格雷。我们的研究在不同分析方法中证实了PRINCE试验主要分析的结果。需要大型随机对照试验来评估我们的发现。Clinicaltrials.gov NCT02506140