Biomedical and Public Health Department, Institut de Recherche en Sciences de la Santé (IRSS), Ouagadougou, 03BP7192, Burkina Faso.
Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montreal, QC, Canada.
BMC Infect Dis. 2020 Jun 26;20(1):449. doi: 10.1186/s12879-020-05169-2.
This study aimed to assess the pharmacokinetic profile of 150 mg rifabutin (RBT) taken every other day (every 48 h) versus 300 mg RBT taken every other day (E.O.D), both in combination with lopinavir/ritonavir (LPV/r), in adult patients with human immunodeficiency virus (HIV) and tuberculosis (TB) co-infection.
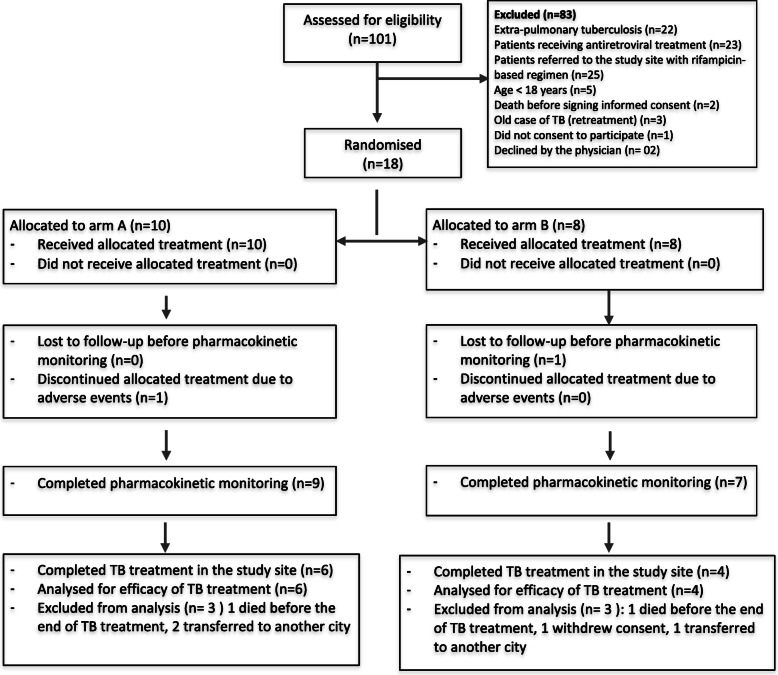
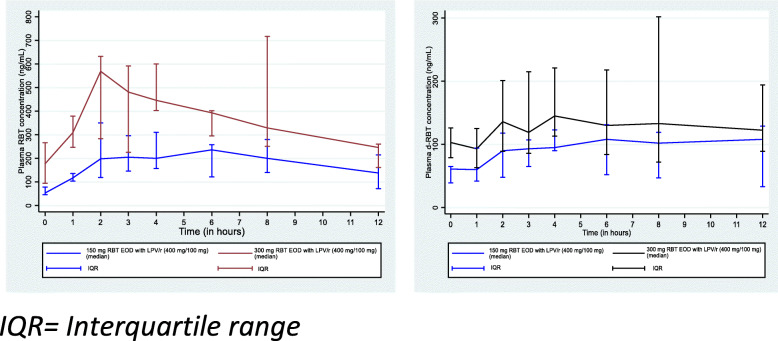
This is a two-arm, open-label, pharmacokinetic, randomised study conducted in Burkina Faso between May 2013 and December 2015. Enrolled patients were randomised to receive either 150 mg RBT EOD (arm A, 9 subjects) or 300 mg RBT EOD (arm B, 7 subjects), both associated with LPV/r taken twice daily. RBT plasma concentrations were evaluated after 2 weeks of combined HIV and TB treatment. Samples were collected just before drug ingestion and at 1, 2, 3, 4, 6, 8, and 12 h after drug ingestion to measure plasma drug concentration using an HPLC-MS/MS assay.
The Cmax and AUC medians in arm A (Cmax = 296 ng/mL, IQR: 205-45; AUC = 2528 ng.h/mL, IQR: 1684-2735) were lower than those in arm B (Cmax = 600 ng/mL, IQR: 403-717; AUC = 4042.5 ng.h/mL, IQR: 3469-5761), with a statistically significant difference in AUC (p = 0.044) but not in Cmax (p = 0.313). No significant differences were observed in Tmax (3 h versus 4 h). Five patients had a Cmax below the plasma therapeutic limit (< 300 ng/mL) in the 150 mg RBT arm, while the Cmax was above this threshold for all patients in the 300 mg RBT arm. Additionally, at 48 h after drug ingestion, all patients had a mycobacterial minimum inhibitory concentration (MIC) above the limit (> 64 ng/mL) in the 300 mg RBT arm, while 4/9 patients had such values in the 150 mg RBT arm.
This study confirmed that the 150 mg dose of rifabutin ingested EOD in combination with LPV/r is inadequate and could lead to selection of rifamycin-resistant mycobacteria.
PACTR201310000629390, 28th October 2013.
本研究旨在评估利福平(RBT)150mg 隔日(每 48 小时)与 300mg 隔日(EOD)两种方案与洛匹那韦/利托那韦(LPV/r)联合用于治疗人类免疫缺陷病毒(HIV)和结核病(TB)合并感染成人患者的药代动力学特征。
这是一项在 2013 年 5 月至 2015 年 12 月期间在布基纳法索进行的、两臂、开放标签、药代动力学、随机研究。纳入的患者被随机分为接受 150mg RBT EOD(臂 A,9 例)或 300mg RBT EOD(臂 B,7 例),均与每日两次的 LPV/r 联合使用。在接受 HIV 和 TB 联合治疗 2 周后,评估 RBT 血浆浓度。在服药前和服药后 1、2、3、4、6、8 和 12 小时采集样本,使用 HPLC-MS/MS 测定法测量血浆药物浓度。
与臂 B(Cmax=600ng/mL,IQR:403-717;AUC=4042.5ng.h/mL,IQR:3469-5761)相比,臂 A(Cmax=296ng/mL,IQR:205-45;AUC=2528ng.h/mL,IQR:1684-2735)的 Cmax 和 AUC 中位数较低,AUC 有统计学显著差异(p=0.044),但 Cmax 无统计学显著差异(p=0.313)。Tmax(3 小时与 4 小时)无显著差异。在 150mg RBT 组中,有 5 名患者的 Cmax 低于血浆治疗下限(<300ng/mL),而在 300mg RBT 组中,所有患者的 Cmax 均高于该阈值。此外,在服药后 48 小时,300mg RBT 组的所有患者的分枝杆菌最低抑菌浓度(MIC)均高于 64ng/mL,而在 150mg RBT 组中,有 4/9 名患者的 MIC 值如此。
本研究证实,利福平 150mg 剂量隔日(EOD)与 LPV/r 联合使用是不足的,可能导致利福霉素耐药分枝杆菌的选择。
PACTR201310000629390,2013 年 10 月 28 日。