San Diego State University and the San Diego State University/University of California San Diego Joint Doctoral Program in Clinical Psychology, California.
University of Connecticut School of Medicine, Farmington.
J Am Acad Child Adolesc Psychiatry. 2021 Mar;60(3):388-397. doi: 10.1016/j.jaac.2020.04.015. Epub 2020 Jun 27.
Disruptive mood dysregulation disorder (DMDD) in DSM, characterized by severe, chronic irritability, currently excludes children <6 years of age. However, capitalizing on a burgeoning developmental science base to differentiate clinically salient irritability in young children may enable earlier identification. The objective of this study was to advance an empirically derived framework for early childhood DMDD (EC-DMDD) by modeling and validating DMDD patterns in early childhood and generating clinically informative, optimized behaviors with thresholds.
Data (N = 425) were from 3 longitudinal assessments of the MAPS Study, spanning preschool (means = 4.7 and 5.5 years) to early school age (mean = 6.8 years). The Multidimensional Assessment Profile of Disruptive Behavior (MAP-DB) Temper Loss scale captured irritability, the Family Life Impairment Scale (FLIS) assessed cross-domain impairment at the preschool time points and the Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS) was used to assess clinical status at early school age. Latent transition analyses differentiated children with EC-DMDD from children with low, transient, or nonimpairing irritability.
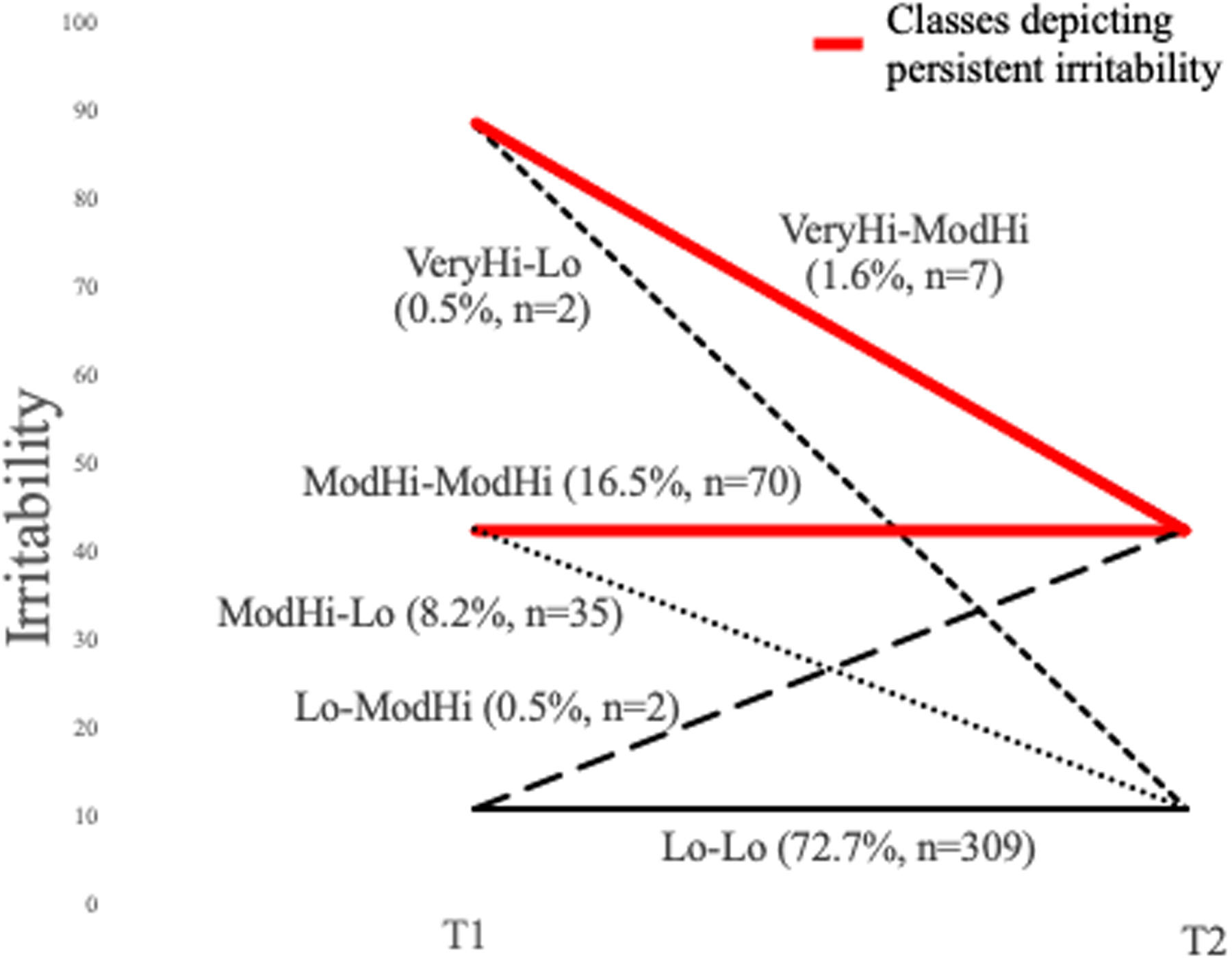
Developmental patterning of irritability proved important for normal:abnormal differentiation. Of children, 27% had initially high irritability, but only two-thirds of these were persistently highly irritable. Thus, "false positives" based on a single screen would be substantial. Yet, "false negatives" are low, as <1% of children with baseline low irritability demonstrated later high irritability. Based on the sequential preschool-age time points, 6.7% of children were identified with EC-DMDD, characterized by persistent irritability with pervasive impairment, similar to prevalence at older ages. Specific behaviors included low frustration tolerance; dysregulated, developmentally unexpectable tantrums; and sustained irritable mood, all of which sensitively (0.85-0.96) and specifically (0.80-0.91) identified EC-DMDD. EC-DMDD predicted irritability-related syndromes (DMDD, oppositional defiant disorder) at early school age better than downward extension of DSM DMDD criteria to preschool age.
These findings provide empirical thresholds for preschool-age clinical identification of DMDD patterns. The results lay the foundation for validation of DMDD in early childhood and inform revision of DSM criteria.
DSM 中的破坏性心境失调障碍(DMDD),其特征为严重、慢性的易激惹,目前排除了年龄<6 岁的儿童。然而,利用新兴的发展科学基础来区分幼儿中具有临床意义的易激惹,可能能够更早地进行识别。本研究的目的是通过对幼儿 DMDD(EC-DMDD)进行建模和验证,并生成具有临床意义的优化行为阈值,从而为其提供一个经验性的框架。
数据(N=425)来自 MAPS 研究的 3 次纵向评估,跨越了学前阶段(平均值=4.7 和 5.5 岁)和小学早期阶段(平均值=6.8 岁)。多维破坏性行为评估量表(MAP-DB)的情绪丧失量表(Temper Loss Scale)捕捉易激惹,家庭生活障碍量表(FLIS)在学前阶段评估跨领域障碍,儿童青少年情感障碍和精神分裂症诊断性定式访谈(K-SADS)在小学早期评估临床状况。潜在转变分析将具有 EC-DMDD 的儿童与易激惹程度较低、短暂或无损伤的儿童区分开来。
易激惹的发展模式对于正常与异常的区分很重要。在儿童中,27%的儿童最初易激惹程度较高,但只有三分之二的儿童持续高度易激惹。因此,基于单次筛查的“假阳性”数量会很大。然而,“假阴性”的数量很低,因为基线易激惹程度较低的儿童中,只有不到 1%的儿童后来表现出高度易激惹。根据学前年龄的顺序,有 6.7%的儿童被诊断为 EC-DMDD,其特征为持续性易激惹和普遍障碍,与较年长儿童的患病率相似。具体行为包括低挫折耐受能力、失调、不符合发育预期的发脾气以及持续的易怒情绪,这些行为都能敏感地(0.85-0.96)和特异性地(0.80-0.91)识别出 EC-DMDD。与 DSM DMDD 标准向下扩展到学前年龄相比,EC-DMDD 能更好地预测小学早期与易激惹相关的综合征(DMDD、对立违抗性障碍)。
这些发现为学龄前儿童 DMDD 模式的临床识别提供了经验阈值。研究结果为早期儿童 DMDD 的验证奠定了基础,并为 DSM 标准的修订提供了信息。