Starr Lauren T, Ulrich Connie M, Junker Paul, Huang Liming, O'Connor Nina R, Meghani Salimah H
NewCourtland Center for Transitions and Health, University of Pennsylvania School of Nursing, Philadelphia, PA, USA.
Center for Bioethics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA.
Am J Hosp Palliat Care. 2020 Oct;37(10):767-778. doi: 10.1177/1049909120934292. Epub 2020 Jun 30.
Early palliative care consultation ("PCC") to discuss goals-of-care benefits seriously ill patients. Risk factor profiles associated with the timing of conversations in hospitals, where late conversations most likely occur, are needed.
To identify risk factor patient profiles associated with PCC timing before death.
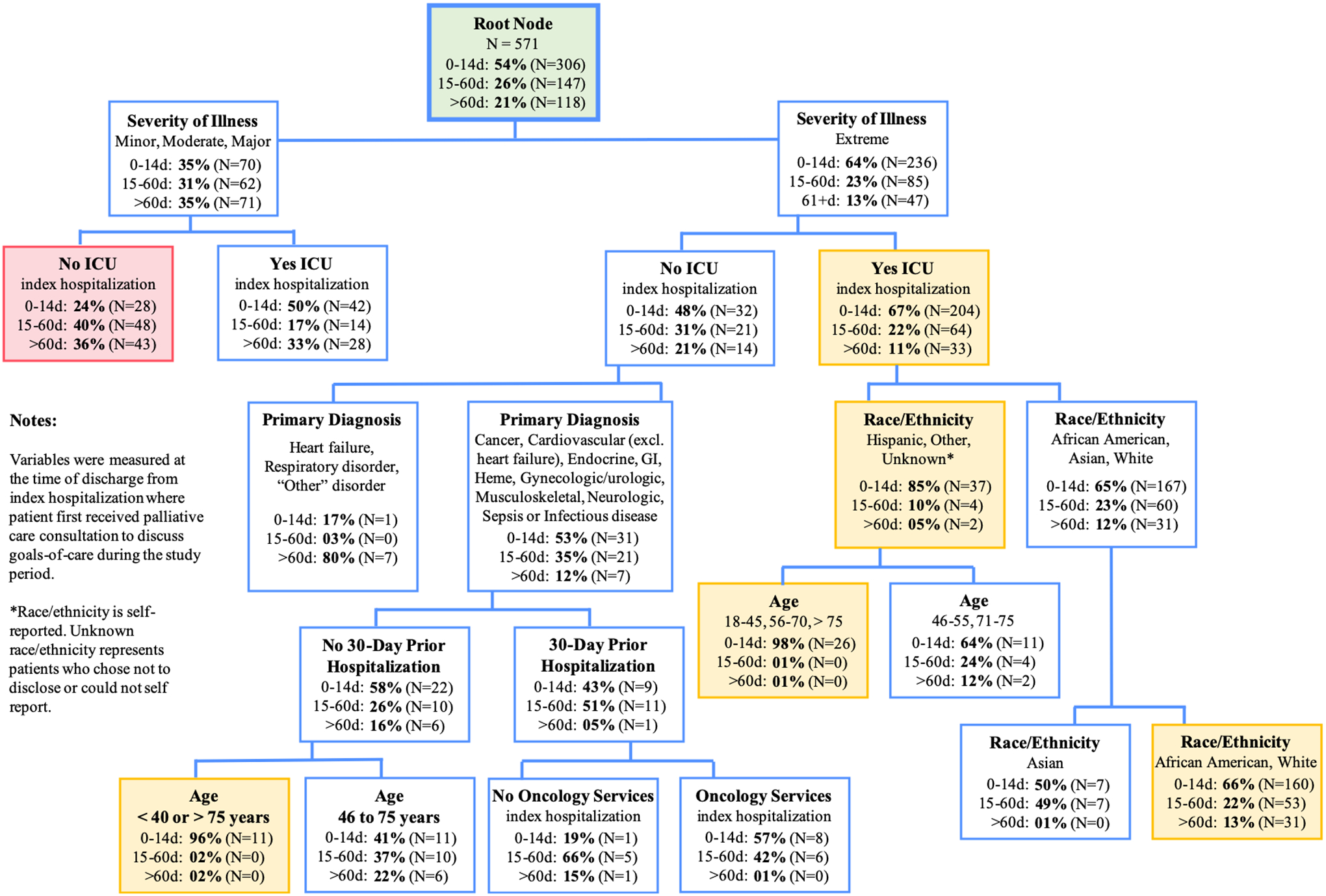
Secondary analysis of an observational study was conducted at an urban, academic medical center. Patients aged 18 years and older admitted to the medical center, who had PCC, and died July 1, 2014 to October 31, 2016, were included. Patients admitted for childbirth or rehabilitationand patients whose date of death was unknown were excluded. Classification and Regression Tree modeling was employed using demographic and clinical variables.
Of 1141 patients, 54% had PCC "close to death" (0-14 days before death); 26% had PCC 15 to 60 days before death; 21% had PCC >60 days before death (median 13 days before death). Variables associated with receiving PCC close to death included being Hispanic or "Other" race/ethnicity intensive care patients with extreme illness severity (85%), with age <46 or >75 increasing this probability (98%). Intensive care patients with extreme illness severity were also likely to receive PCC close to death (64%) as were 50% of intensive care patients with less than extreme illness severity.
A majority of patients received PCC close to death. A complex set of variable interactions were associated with PCC timing. A systematic process for engaging patients with PCC earlier in the care continuum, and in intensive care regardless of illness severity, is needed.
早期姑息治疗咨询(“PCC”)有助于与重症患者讨论治疗目标。我们需要了解与医院中谈话时机相关的风险因素概况,因为晚期谈话最有可能在医院发生。
确定与死亡前PCC时机相关的风险因素患者概况。
在一家城市学术医疗中心对一项观察性研究进行二次分析。纳入2014年7月1日至2016年10月31日期间入住该医疗中心、接受过PCC且已死亡的18岁及以上患者。排除因分娩或康复入院的患者以及死亡日期不明的患者。使用人口统计学和临床变量进行分类与回归树建模。
在1141名患者中,54%在“临近死亡”时接受了PCC(死亡前0 - 14天);26%在死亡前15至60天接受了PCC;21%在死亡前>60天接受了PCC(中位时间为死亡前13天)。与临近死亡时接受PCC相关的变量包括西班牙裔或“其他”种族/族裔、病情极其严重的重症监护患者(85%),年龄<46岁或>75岁会增加这种可能性(98%)。病情极其严重的重症监护患者也很可能在临近死亡时接受PCC(64%),病情不太严重的重症监护患者中有50%也是如此。
大多数患者在临近死亡时接受了PCC。一组复杂的变量相互作用与PCC时机相关。需要一个系统的流程,以便在护理连续过程中更早地让患者接受PCC,并且无论病情严重程度如何,在重症监护中也是如此。