College of Public Health and Human Sciences, Oregon State University, Corvallis.
Division of Oncological Sciences, Oregon Health & Science University, Portland.
JAMA Netw Open. 2020 Jun 1;3(6):e207227. doi: 10.1001/jamanetworkopen.2020.7227.
Interval breast cancers (IBCs) are cancers that emerge after a mammogram with negative results but before the patient's next scheduled screening. Interval breast cancer has a worse prognosis than cancers detected by screening; however, it is unknown whether the length of the interscreening period is associated with prognostic features and mortality.
To compare the prognostic features and mortality rate of women with IBCs diagnosed within 1 year or between 1 and 2.5 years of a mammogram with negative results with the prognostic features and mortality rate of women with breast cancers detected by screening.
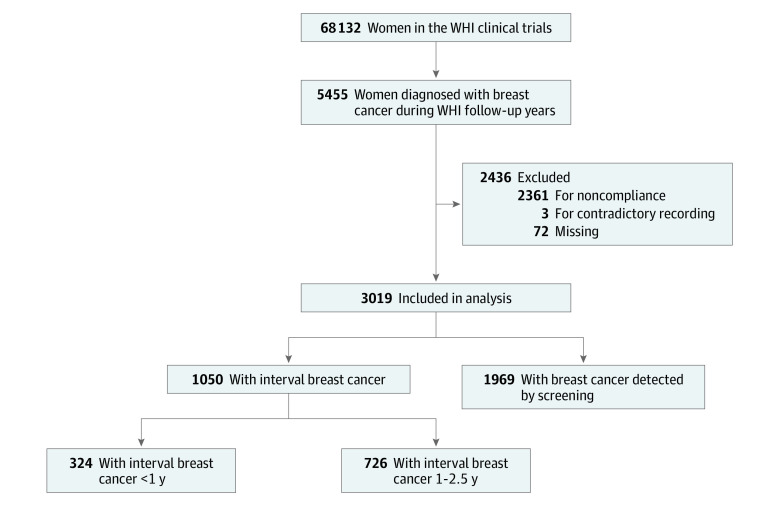
DESIGN, SETTING, AND PARTICIPANTS: This cohort study used mammography data, tumor characteristics, and patient demographic data from the Women's Health Initiative study, which recruited participants from 1993 to 1998 and followed up with participants for a median of 19 years. The present study sample for these analyses included women aged 50 to 79 years who participated in the Women's Health Initiative study and includes data collected through March 31, 2018. There were 5455 incidents of breast cancer; only 3019 women compliant with screening were retained in analyses. Statistical analysis was performed from October 25, 2018, to November 24, 2019. Breast cancers detected by screening and IBCs were defined based on mammogram history, date of last mammogram, type of visit, and results of examination. Interval breast cancers were subdivided into those occurring within 1 year or between 1 and 2.5 years after the last protocol-mandated mammogram with negative results.
The primary outcome of this study was breast cancer-specific mortality for each case of breast cancer detected by screening and IBCs detected within 1 year or between 1 and 2.5 years from a mammogram with negative results. Secondary outcomes included prognostic and tumor characteristics for each group. Comparisons between groups were made using the t test, the χ2 test, and Fine-Gray multivariable cumulative incidence regression analyses.
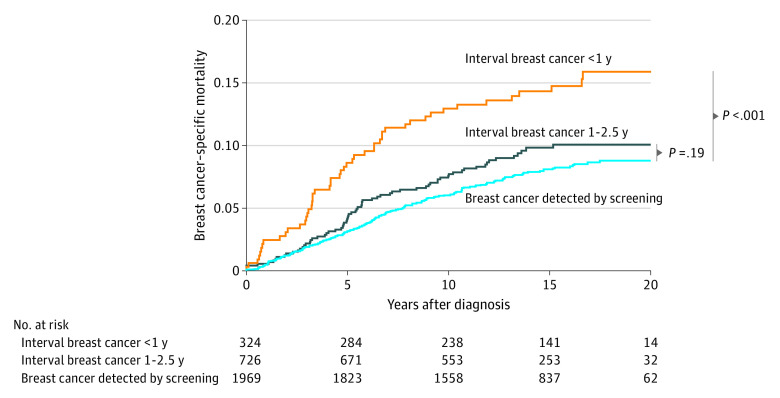
Among the 3019 participants in this analysis, all were women with a mean (SD) age of 63.1 (6.8) years at enrollment and 68.5 (7.1) years at diagnosis. A total of 1050 cases of IBC were identified, with 324 (30.9%) diagnosed within 1 year from a mammogram with negative results and 726 (69.1%) diagnosed between 1 and 2.5 years after last mammogram with negative results. The remaining 1969 cases were breast cancers detected by screening. Interval breast cancers diagnosed within 1 year from a mammogram with negative results had significantly more lobular histologic characteristics (13.0% vs. 8.1%), a larger tumor size (1.97 cm vs 1.43 cm), a higher clinical stage (28.4% vs 17.3% regional and 3.7% vs 0.6% distant), and more lymph node involvement (27.1% vs 17.0%) than cancers detected by screening. Unadjusted breast cancer-specific mortality hazard ratios were significantly higher for IBCs diagnosed within 1 year from a mammogram with negative results compared with breast cancers detected by screening (hazard ratio, 1.92; 95% CI, 1.39-2.65). Higher breast cancer-specific mortality remained statistically significant for IBCs diagnosed within 1 year after adjusting for trial group, molecular subtype, waist to hip ratio, histologic characteristics, and either tumor size (hazard ratio, 1.46; 95% CI, 1.03-2.08) or lymph node involvement (hazard ratio, 1.44; 95% CI, 1.03-2.01). However, significance was lost when tumor size and lymph node involvement were both included in the model (hazard ratio, 1.34; 95% CI, 0.96-1.88). Interval breast cancers diagnosed between 1 and 2.5 years from a mammogram with negative results were not different from breast cancers detected by screening based on prognostic factors or mortality.
Women with IBCs diagnosed within 1 year of negative mammogram results overall were associated with worse survival than women with breast cancers detected by screening. These differences in survival may be due to a uniquely aggressive biology among IBC cases.
重要性:间隔期乳腺癌(IBC)是指在阴性乳房 X 光检查后至下一次预定筛查前出现的癌症。间隔期乳腺癌的预后比通过筛查检测到的癌症差;然而,尚不清楚筛查间期的长度是否与预后特征和死亡率相关。
目的:比较在阴性乳房 X 光检查后 1 年内或 1 至 2.5 年内诊断为 IBC 的女性与通过筛查检测到的乳腺癌的女性的预后特征和死亡率。
设计、设置和参与者:这项队列研究使用了妇女健康倡议研究中的乳房 X 光数据、肿瘤特征和患者人口统计学数据,该研究于 1993 年至 1998 年招募参与者,并对参与者进行了中位数为 19 年的随访。本研究的样本包括年龄在 50 至 79 岁之间参加妇女健康倡议研究的女性,并包含截至 2018 年 3 月 31 日的数据。有 5455 例乳腺癌病例;仅保留了 3019 名符合筛查要求的女性进行分析。统计分析于 2018 年 10 月 25 日至 2019 年 11 月 24 日进行。通过乳房 X 光检查史、最后一次乳房 X 光检查日期、就诊类型和检查结果来定义通过筛查检测到的乳腺癌和 IBC。间隔期乳腺癌分为在最后一次协议规定的阴性乳房 X 光检查后 1 年内或 1 至 2.5 年内发生的病例。
主要结果和措施:本研究的主要结局是通过筛查检测到的乳腺癌和在阴性乳房 X 光检查后 1 年内或 1 至 2.5 年内诊断为 IBC 的每个病例的乳腺癌特异性死亡率。次要结局包括每个组的预后和肿瘤特征。通过 t 检验、卡方检验和 Fine-Gray 多变量累积发生率回归分析比较组间差异。
结果:在本分析的 3019 名参与者中,所有参与者的平均(SD)年龄为 63.1(6.8)岁,入组时为 68.5(7.1)岁,诊断时为 68.5(7.1)岁。共发现 1050 例 IBC,其中 324 例(30.9%)在阴性乳房 X 光检查后 1 年内诊断,726 例(69.1%)在最后一次阴性乳房 X 光检查后 1 至 2.5 年内诊断。其余 1969 例为通过筛查检测到的乳腺癌。在阴性乳房 X 光检查后 1 年内诊断为 IBC 的病例,其组织学特征更具小叶特征(13.0%比 8.1%),肿瘤大小更大(1.97cm 比 1.43cm),临床分期更高(28.4%比 17.3%局部和 3.7%比 0.6%远处),淋巴结受累更多(27.1%比 17.0%),而通过筛查检测到的乳腺癌。未调整的乳腺癌特异性死亡率危险比对于在阴性乳房 X 光检查后 1 年内诊断为 IBC 的病例明显高于通过筛查检测到的乳腺癌(危险比,1.92;95%CI,1.39-2.65)。在调整试验组、分子亚型、腰臀比、组织学特征以及肿瘤大小(危险比,1.46;95%CI,1.03-2.08)或淋巴结受累(危险比,1.44;95%CI,1.03-2.01)后,较高的乳腺癌特异性死亡率仍然具有统计学意义。然而,当肿瘤大小和淋巴结受累均纳入模型时,意义丧失(危险比,1.34;95%CI,0.96-1.88)。在阴性乳房 X 光检查后 1 至 2.5 年内诊断为 IBC 的病例与通过筛查检测到的乳腺癌的预后因素或死亡率无差异。
结论和相关性:总体而言,在阴性乳房 X 光检查结果后 1 年内诊断为 IBC 的女性的生存预后明显比通过筛查检测到的乳腺癌的女性差。这些生存差异可能是由于 IBC 病例具有独特的侵袭性生物学。