Kidney Health Service, Royal Brisbane and Women's Hospital, Herston, Qld, Australia.
Pathology Department, Royal Brisbane and Women's Hospital, Herston, Qld, Australia.
Transpl Infect Dis. 2020 Dec;22(6):e13399. doi: 10.1111/tid.13399. Epub 2020 Jul 14.
BK virus (BKPyV) nephropathy occurs in 1%-10% of kidney transplant recipients, with suboptimal therapeutic options.
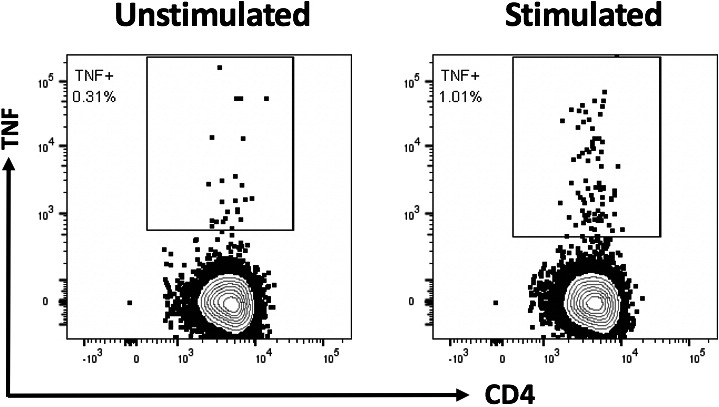
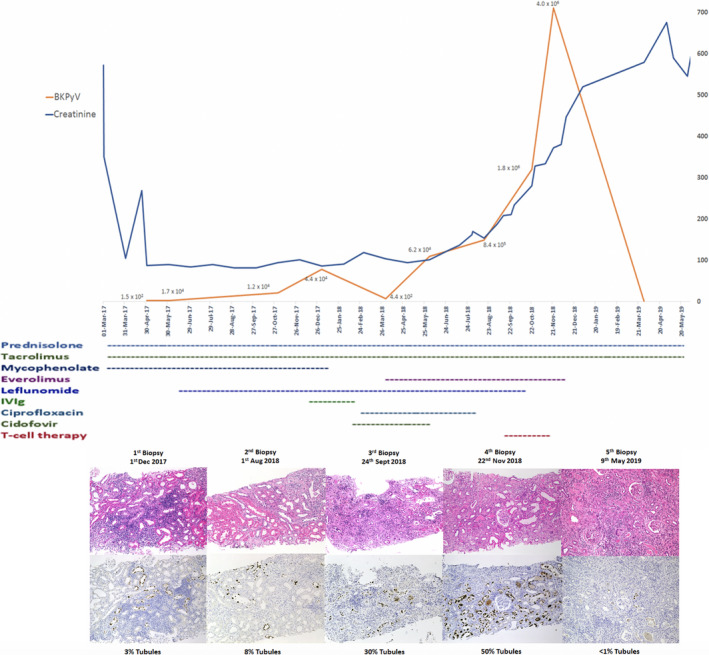
A 54-year-old woman received a transplant in March 2017. BKPyV was detected at 1.5 × 10 copies/mL within a month, necessitating halving of mycophenolate and addition of leflunomide. Allograft histology in December showed polyomavirus nephropathy treated with intravenous immunoglobulin and cessation of mycophenolate. In February 2018, cidofovir and ciprofloxacin were commenced. In April, tacrolimus was reduced while introducing everolimus. A second graft biopsy in August showed increasing polyoma virus infection and a subsequent biopsy in September for worsening renal function showed 30% of tubular reactivity for simian virus 40 (SV40). Allogeneic BKPyV-reactive T cells were generated from the patient's daughter and infused over 10 sessions starting late September. The fourth allograft biopsy in November 2018 demonstrated involvement of BKPyV in 50% of tubules. Allograft function continued to decline, requiring hemodialysis from December 2018. Allograft nephrectomy after 6 months showed <1% SV40 in preserved tubules and 80% interstitial fibrosis.
We conclude that the T-cell adoptive immunotherapy reduced BKPyV load significantly despite extensive infection, but attendant fibrosis and tubular atrophy led to graft failure. Early intervention with T-cell therapy may prove efficacious in BKPyV nephropathy.
BK 病毒(BKPyV)肾病发生于 1%-10%的肾移植受者中,治疗方法选择有限。
一名 54 岁女性于 2017 年 3 月接受移植。1 个月内 BKPyV 检测值为 1.5×10 拷贝/ml,需要将吗替麦考酚酯减半并加用来氟米特。12 月的移植肾活检显示为多瘤病毒肾病,给予静脉注射免疫球蛋白和停用吗替麦考酚酯治疗。2018 年 2 月开始使用更昔洛韦和环丙沙星。4 月时,减少他克莫司的用量,同时引入依维莫司。8 月的第二次移植肾活检显示多瘤病毒感染加重,9 月因肾功能恶化进行的再次活检显示 30%的肾小管对猿猴病毒 40(SV40)呈反应性。从患者女儿中生成同种异体 BKPyV 反应性 T 细胞,并从 9 月底开始分 10 次输注。2018 年 11 月第 4 次移植肾活检显示 50%的肾小管受累 BKPyV。移植物功能持续下降,2018 年 12 月开始血液透析。移植肾切除术后 6 个月的检查显示,保存的肾小管中 SV40<1%,间质纤维化 80%。
我们得出结论,尽管感染广泛,但 T 细胞过继免疫治疗显著降低了 BKPyV 载量,但随之而来的纤维化和肾小管萎缩导致移植物衰竭。早期进行 T 细胞治疗可能对 BKPyV 肾病有效。