ADB Building, Boehringer Ingelheim Pharma GmbH & Co. KG, Biberach, Germany and Hochschule Biberach, University of Applied Sciences, Germany (E.B.).
The Medical Department, Boehringer Ingelheim France SAS, Reims (T.D.).
Stroke. 2020 Aug;51(8):2322-2331. doi: 10.1161/STROKEAHA.119.028396. Epub 2020 Jul 2.
BACKGROUND/PURPOSE: Expert guidelines specify no upper age limit for alteplase for thrombolysis of acute ischemic stroke (AIS) but, until recently, European regulatory criteria restricted its use to patients aged 18 to 80 years. We performed pooled analyses of randomized controlled trial (RCT) and registry data to evaluate the benefit-risk profile of alteplase for AIS among patients aged >80 years to support a regulatory application to lift the upper age restriction.
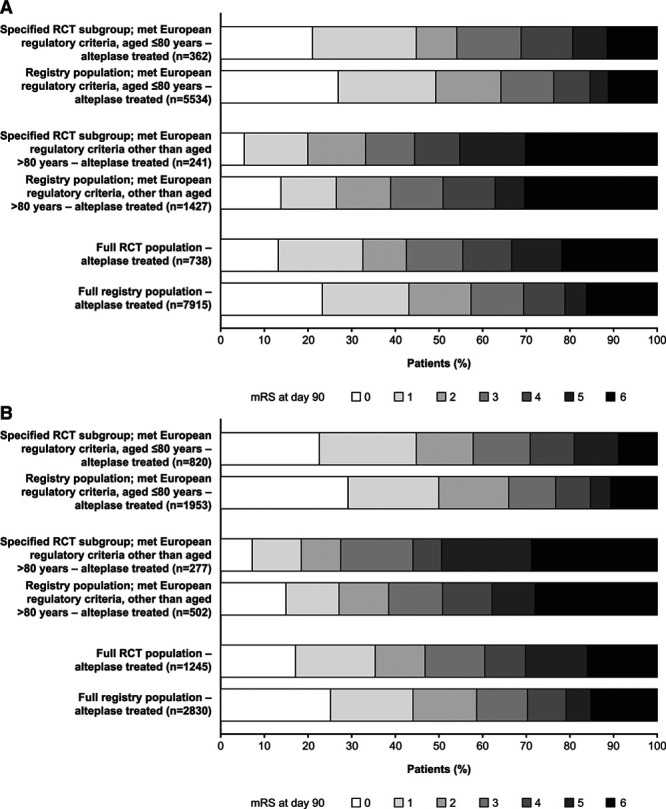
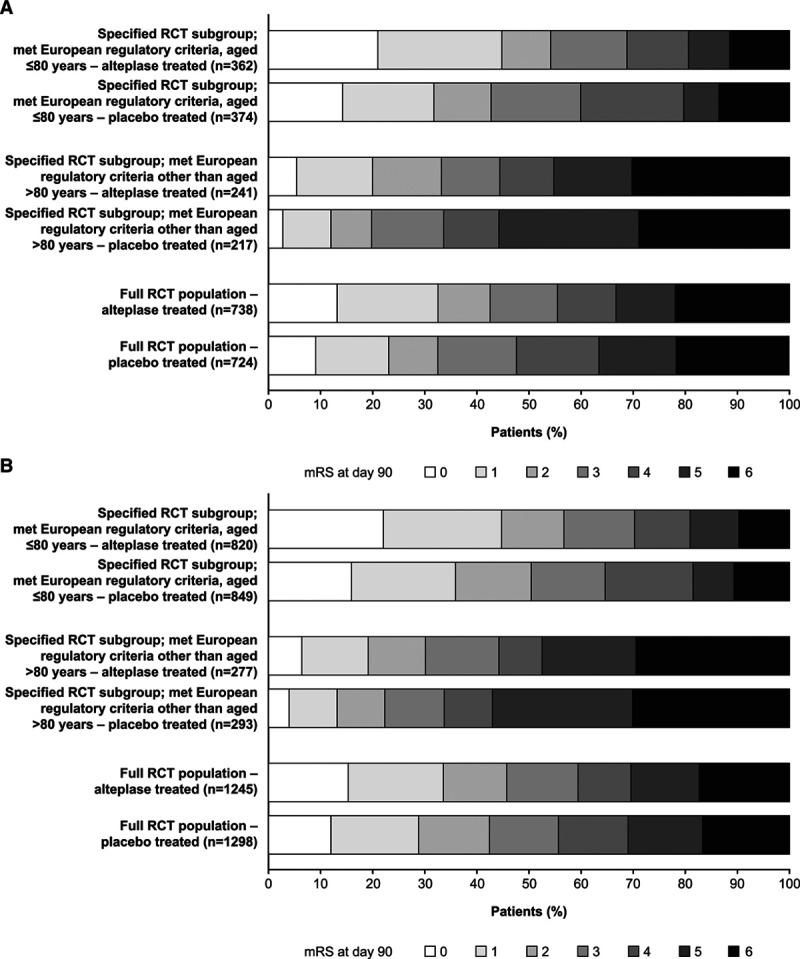
Individual patient data were evaluated from 7 randomized trials of alteplase (0.9 mg/kg) versus placebo or open control for AIS, and the European SITS-UTMOST registry database. Clinical outcomes, including good functional outcome (score 0-1, modified Rankin Scale day 90 or Oxford Handicap Score day 180), were evaluated in the full RCT and registry populations, and specified age-based subgroups (≤80 or >80 years) who met existing European regulatory criteria for alteplase, excluding upper age restriction.
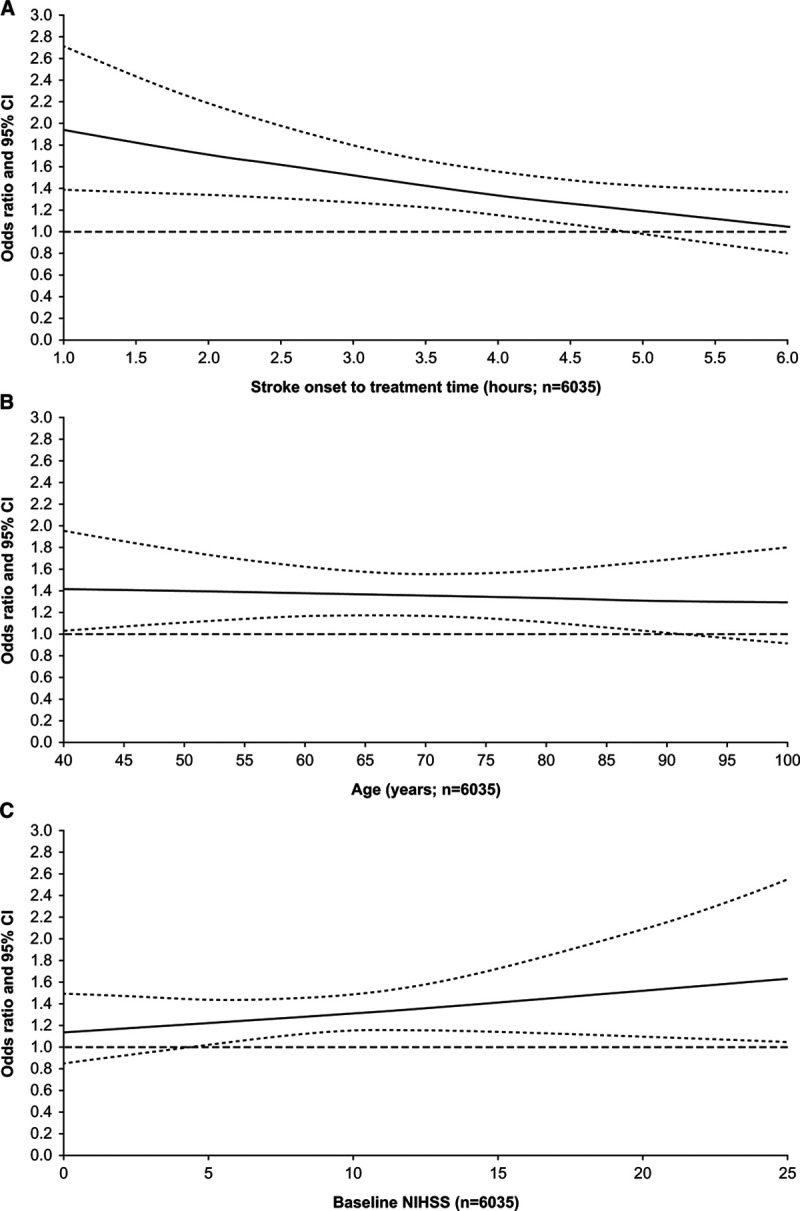
Regardless of treatment allocation, 90-day mortality was lower among RCT patients aged ≤80 versus >80 years who otherwise met existing European regulatory criteria (246/2405 [10.2%] versus 307/1028 [29.9%], respectively). Among patients aged >80 years, alteplase versus placebo was associated with a higher proportion of good stroke outcome (modified Rankin Scale score 0-1; 99/518 [19.1%] versus 67/510 [13.1%]; =0.0109) and similar 90-day mortality (153/518 [29.5%] versus 154/510 [30.2%]; =0.8382). The odds of a good stroke outcome following alteplase allocation in the full RCT population were independent of age (=0.7383). Good stroke outcome was reported for almost half (4821/11 169 [43.2%]) of the patients who received alteplase in routine practice. Outcomes in routine practice supported those achieved in RCTs.
Alteplase for AIS has a positive benefit-risk profile among patients aged >80 years when administered according to other regulatory criteria. Alteplase for AIS should be evaluated on an individual benefit-risk basis.
背景/目的:专家指南规定,阿替普酶溶栓治疗急性缺血性脑卒中(AIS)没有年龄上限,但直到最近,欧洲监管标准仍将其使用限制在 18 至 80 岁的患者。我们对随机对照试验(RCT)和登记研究的数据进行了汇总分析,以评估阿替普酶治疗年龄>80 岁的 AIS 患者的获益-风险特征,以支持解除年龄上限的监管申请。
从 7 项阿替普酶(0.9mg/kg)与安慰剂或开放对照治疗 AIS 的随机试验和欧洲 SITS-UTMOST 登记数据库中评估了个体患者数据。在 RCT 和登记人群中评估了临床结局,包括良好的功能结局(90 天改良 Rankin 量表评分 0-1 分或 180 天牛津残疾评分),并在符合现有欧洲阿替普酶监管标准的特定年龄亚组(≤80 岁或>80 岁)中进行了评估,排除了年龄上限。
无论治疗分配如何,符合现有欧洲监管标准但年龄>80 岁的 RCT 患者 90 天死亡率低于年龄≤80 岁的患者(246/2405[10.2%]与 307/1028[29.9%])。在年龄>80 岁的患者中,阿替普酶与安慰剂相比,良好的卒中结局(改良 Rankin 量表评分 0-1 分)的比例更高(99/518[19.1%]与 67/510[13.1%];=0.0109),90 天死亡率相似(153/518[29.5%]与 154/510[30.2%];=0.8382)。在 RCT 全人群中,阿替普酶治疗后良好的卒中结局与年龄无关(=0.7383)。在常规实践中,接受阿替普酶治疗的患者中,几乎有一半(4821/11169[43.2%])报告了良好的卒中结局。常规实践中的结局支持 RCT 中的结局。
在符合其他监管标准的情况下,阿替普酶治疗年龄>80 岁的 AIS 患者具有良好的获益-风险特征。阿替普酶治疗 AIS 应根据个体获益-风险进行评估。